

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Syncope is a common clinical problem in the emergency department (ED), accounting for 3-5% of all ED visits and 1-6% of all hospital admissions.1-5 Moreover, it has a substantial financial impact on health care and imposes a significant socioeconomic burden.6,7 The total annual costs for syncope-related hospital admissions are estimated to be $ 2.4 billion in the United States.8
The evaluation of syncope is often not standardized and ineffective.9,10 Despite the recent publication of guidelines regarding appropriate and structured evaluation of syncope,2,11,12 these guidelines have not been widely disseminated and are sometimes difficult to apply in clinical practice.9,13 Even hospital-based education may be insufficient to ensure optimal evaluation. As a result, inappropriate diagnostic tests and unnecessary hospitalizations are frequent in the processes of diagnosing and managing syncope.14
Recently, several studies reported that the implementation of standardized care pathways significantly improved diagnostic yields and reduced the rate of hospital admissions as well as overall medical costs related to syncope evaluation.13,15-19 However, to our knowledge, few have reported on improvements in the quality of syncope evaluation as a result of the implementation of standardized approaches in hospitals of different settings with limited medical resources in Asia.19
The aim of this study was to examine the effectiveness of a simple, standardized ED protocol comprising an educational program, risk stratification, hospital order sets, and establishment of a syncope observational unit at a tertiary-care hospital in South Korea.
MATERIALS AND METHODS
Study design and setting
This study was a prospective, nonrandomized study conducted at Samsung Medical Center, a 1900-bed, tertiary-care teaching hospital, with an annual ED census of 67000 visits, in Seoul, South Korea. We compared two specific periods: a 12-month observation period before the implementation of a standardized ED protocol (control group, January-December 2009) and a 10-month intervention period after protocol implementation (intervention group, March-December 2010). The study was approved by the hospital's institutional review board. Informed consent was obtained from all study participants or their legal designates.
Selection of participants
Consecutive patients aged 18 years or older presenting to the ED with syncope were recruited to participate in the study. Syncope was defined as a sudden, transient loss of consciousness with spontaneous recovery due to transient global cerebral hypoperfusion.2,18 Exclusion criteria were lack of consent, previous enrollment in other studies, and non-syncopal episodes such as lightheadedness, vertigo, hypoglycemia, seizure or stroke.
Syncope evaluation in the observation period
Patients who visited the ED with syncope were evaluated without standardized guidelines or educational programs on proper syncope evaluation. There were no ED protocols for syncope or syncope observational unit. Clinical decisions were made largely by the ED resident or attending physician for each case.
Syncope evaluation in the intervention period
Between January and February 2010, we conducted an educational program for physicians-in-training and ED faculty, including a 1-hour lecture. The educational program covered an initial evaluation for syncope, risk stratification, a standardized ED protocol, important electrocardiogram (ECG) findings and several clinical cases. The educational program and the ED protocol were largely based on the 2009 European Society of Cardiology (ESC) guidelines.2 Risk stratification was conducted by initial history taking and evaluation in the ED. We defined "high risk" according to the ESC guidelines, summarized as follows: 1) severe structural heart disease or coronary heart disease, (1) heart failure, (2) low left ventricular ejection fraction, or (3) previous myocardial infarction; 2) clinical or ECG features suggesting arrhythmic syncope, (1) syncope during exertion or supine, (2) palpitations at the time of syncope, (3) family history of sudden cardiac death, (4) non-sustained ventricular tachycardia, (5) bifascicular-block or intraventricular conduction abnormalities with QRS duration ≥120 ms, (6) inadequate sinus bradycardia (<50 bpm) or sinoatrial block in the absence of negative chronotropic medications or physical training, (7) pre-excited QRS complex, (8) prolonged or short QT interval, (9) Brugada pattern, (10) ECG findings suggestive of arrhythmogenic right ventricular cardiomyopathy; or 3) important comorbidities (severe anemia, electrolyte disturbance). "Low risk" was defined as follows: 1) age <50 years, 2) no previous history of cardiovascular disease, 3) symptoms consistent with reflex-mediated or vasovagal syncope, 4) normal cardiovascular examination, and 5) normal ECG findings.18 If patients were neither low nor high risk, they were categorized as "intermediate risk".
When patients visited the ED due to syncope, the ED physician obtained their clinical history and performed a physical examination. After the ECG was performed, the ED physician stratified subjects into specific risk groups. Hospital order sets were provided according to risk. All order sets included regular vital sign checking, postural blood pressure evaluation, and order for initial evaluation at the ED. The order set for the low-risk group included a complete blood count and serum electrolytes (with or without blood chemistries depending on the physician's decision). For the intermediate and high-risk groups, blood chemistries were routinely assessed (glucose, blood urea nitrogen, creatinine, liver function tests). Continuous ECG monitoring, cardiac enzymes, and cardiologic consultation were added for the high-risk group. The sets were modified or tests were added depending on the patient's history, condition, or if further tests were deemed necessary by the physician.
Low-risk patients were discharged without further investigation in the ED and referred to the outpatient department (OPD) for additional evaluation, if needed. Outpatient follow-up was available for both the control and the intervention groups. We also recommended early follow-up and investigation for intermediate-risk patients who were stable and did not have any significant findings in the ED. All patients of high risk and patients of intermediate risk with significant findings in the ED were placed in a syncope observational unit in the ED, which consisted of two beds with continuous monitoring equipment for prompt and intensive monitoring of patients of high or intermediate risk. Unfortunately, the observational unit shared beds with a previously existing observational unit for coronary syndrome patients because of a severe overcrowding problem in the ED. However, during the observation period, no monitoring section was allowed to be used exclusively, and the ED bed-management protocol for patients with syncope, including decisions about which patients to monitor, was dependent on the physicians in charge without formal risk stratification. Additional tests including echocardiography, head-up tilt test, Holter monitoring, treadmill test, brain imaging, electroencephalography and carotid Doppler were performed at the ED or the OPD, according to the clinical decision of the emergency physicians or cardiologists based on the current ESC guidelines.2 Coronary angiography, electrophysiological study and implantable loop recorder evaluations were performed after hospitalization, if appropriate. The on-duty cardiologist made decisions regarding whether or not to admit individual patients.
There were no differences in medico-sociological conditions or hospital policies between the two periods, except the protocol for evaluation of syncope.
End points and data collection
We evaluated two primary end points: hospital admission rates and medical costs. When patients were hospitalized after follow-up visits at the OPD, these hospitalizations were also included. Costs were calculated during diagnostic evaluation according to hospital accounting reports. Indirect costs such as loss of earnings or costs paid by patients at other hospitals were not evaluated. Costs are expressed in Korean won (KRW), the currency of South Korea (approximately 1000 won=1 United States dollar).
The secondary end points were ED length of stay (LOS), hospital LOS, rate of certain diagnosis, all-cause mortality and recurrent syncope during six-month follow-up. Certain diagnosis was recognized when the initial evaluation lead to a diagnosis based on symptoms, signs, ECG findings or when a suspected diagnosis was confirmed by direct testing.18
We prospectively collected data on each patient's demographic factors, comorbidities, family history, previous syncopal episodes, presenting symptoms, risk stratification, syncope-related trauma, as well as diagnostic tests and procedures. The ED occupancy rate was also calculated in terms of enrolled patient visits.20 Diagnoses were established based on previously described criteria:2,21 neurally mediated, orthostatic hypotension, cardiac arrhythmia, structural cardiac, cerebrovascular, and unknown causes of syncope. Bony fractures, cerebral concussions and lacerations caused by syncopal episodes were defined as significant trauma. At the 6-month follow-up, recurrences of syncope and survival data were obtained through telephone interviews by a trained nurse coordinator.
Power estimates and statistics
We expected to recruit 100 patients for each period according to previous data. If we assumed that a 20% difference in the hospital admission rate (30% vs. 10%) would be considered significant, the statistical power would be 92.5% (alpha error, 0.05). For a 15% difference in the admission rate, the estimated statistical power was 74.4 percent.
Continuous variables were expressed as the mean±stan-dard deviation or the median (interquartile range, IQR). These variables were compared using Student's t-test or Wilcoxon's rank-sum test, while categorical variables were compared by chi-square test or Fisher's exact test. A multiple logistic regression analysis was used to estimate the adjusted odds ratio for hospitalization. A multiple linear regression analysis was also performed to predict independent factors associated with total medical costs. In those multivariate models, we adjusted variables including age, gender, risk strata and syncope-related trauma. Stata version 12.0 (Stata Corp LP, College Station, TX, USA) was used to perform the statistical analyses, and two-tailed p-values <0.05 were considered to be significant.
RESULTS
Characteristics of the study subjects
A total of 281 eligible patients were identified. Among them, 37 patients who did not consent to participate were excluded (15 patients in the control group, 22 patients in the intervention group). Finally, 244 patients were enrolled in this study (116 patients in the control group and 128 patients in the intervention group).
There were no significant differences in baseline characteristics between the two groups with the exception of age. The mean age of the intervention group was older than that of the control group (52.3±17.2 vs. 46.4±18.4, p=0.01). High-risk patients were slightly more frequent in the intervention group, but this difference was not statistically significant (18.7% vs. 10.3%, p=0.16). Neurally mediated syncope was the most common diagnosis in both groups (65.5% vs. 62.9%, p=0.35). The ED occupancy rates were very high for both periods (Table 1).
Fifty-five patients (47.4%) in the control group and 75 patients (58.5%) in the intervention group visited the OPD after visiting the ED. The total numbers of OPD visits during the evaluation of syncope were 147 and 127, respectively. In the intervention group, the syncope unit treated a total of 37 patients (28.9%).
Diagnostic tests for the evaluation of syncope
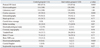
Postural blood pressure measurement was more frequently performed in the intervention group than the control group (97.6% vs. 87.9%, p=0.003). However, the use of cardiac enzymes and electroencephalography were lower in the intervention group than the control group, respectively (42.9% vs. 56.0%, p=0.041; 2.3% vs. 8.6%, p=0.029). The frequencies of other diagnostic tests were not significantly different between the two groups (Table 2).
Primary endpoint-hospital admission rate
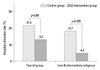
The admission rate decreased by 8.3% in the intervention group [unadjusted odds ratio (OR) 0.55, 95% confidence interval (CI) 0.28-1.09, p=0.08]. In particular, the admission rate was reduced by 13.4% for low or intermediate-risk patients (unadjusted OR 0.22, 95% CI 0.08-0.63, p=0.005) (Fig. 1). In the multivariate logistic regression test, membership in the intervention group was associated with a reduction in hospitalization after adjustment for potential confounding factors (OR 0.31, 95% CI 0.13-0.70, p=0.005) (Table 3).
Primary endpoint-medical cost
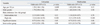
There was a substantial cost reduction of about 30% in the intervention period (369000 KRW, IQR 240000-602000 KRW), compared with the control period (542000 KRW, IQR 316000-1185000 KRW). This difference was especially prominent when we compared the costs paid by low- or intermediate-risk patients, the costs at the ED, the costs paid by patients revisiting the OPD and the costs for diagnostic tests (Table 4). In the multivariate linear regression analysis of medical costs, membership in the intervention group was associated with decreased costs (coefficient -712000 KRW, 95% CI -1341000 to -83000 KRW, p=0.027) (Table 5).
Secondary endpoints
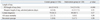
The ED LOS was significantly reduced in the intervention group, although the hospital LOS was not different between the two groups (median: 4.6 hours vs. 3.4 hours). There was an increasing trend in the rate of certain diagnosis in the intervention group, but it was not statistically significant.
During the six-month follow-up, three deaths were reported (1 patient in the control group and 2 patients in the intervention group). These were not unexpected events, as they were deaths due to malignancies. Recurrent syncopal events were reported for 3 patients (one in the control group and two in the intervention group). Because very few adverse events were reported, we were unable to compare the two groups regarding this measure, although we did evaluate the outcomes of all patients through OPD visits or telephone interviews (Table 6).
DISCUSSION
Although syncope is a commonly presenting symptom, the evaluation of syncope in the ED is often challenging and time-consuming, and may incur unnecessary health care costs and delays in the diagnostic process.6,7,22 In our study, admission rates, medical costs and ED LOS were significantly reduced after the implementation of systematic approaches for syncope evaluation. We observed outcome improvements, particularly in low or intermediate-risk patients. These results have important clinical implications, as inappropriate admission, medical costs, and ED length of stay in the low and intermediate-risk patients were significantly reduced. Our results provide evidence for the importance of standardized evaluation and care for syncope in the ED.
Education alone may be insufficient to modify physician behavior, as local hospital education programs often do not lead to notable changes in the evaluation of syncope.9,23 We hypothesized that a simple, organized approach would help to overcome this barrier. The educational program and protocol used in this study focused on initial risk stratification and evaluation in the ED. We also recommended that ED physicians use a hospital order set according to patient risk.
The effectiveness of a standardized order set in the evaluation of syncope has not yet been demonstrated. Such use may ensure that necessary procedures are performed and may allow for new practice changes.24 Regarding diagnostic tests, we hypothesized that a standardized order set would have the positive effect of reducing the use of less specific tests for diagnosis and encourage the measurement of postural blood pressure during initial investigations. Our standardized order sets, however, were limited in the initial evaluation in the ED and should be optimized according to current evidence. Further study of a well-organized hospital order set and an extended decision-making system for additional testing are needed.
Although several methods for risk stratification have demonstrated prognostic value, there is no clear evidence that any method directly improves diagnostic accuracy or reduces costs; moreover, risk stratification methods may, in fact, increase costs.2,15,18,25-27 However, risk stratification may be useful if clinical evaluation is appropriately performed, depending on risk. Shen, et al.18 showed that focused evaluation of intermediate-risk patients, based on a specific syncope unit, significantly improved diagnostic yield and reduced hospital admission.
The creation of formal syncope units may increase diagnostic yield and prevent unnecessary admissions and testing.15,17,18,28 In our study, we were unable to fully evaluate the effectiveness of a dedicated syncope unit, because our unit was not exclusively used for syncope patients, and most tests and specialist assessments could be performed in other areas of the ED if clinically indicated.
One change that was made as a result of our study was the modification of the ED bed management policy. There was no established protocol for bed assignment of syncope patients during the control period, despite ED overcrowding. We hypothesized that the implementation of such a protocol would enable more rapid and safe monitoring and evaluation of high-risk or intermediate-risk patients. However, we anticipate that such protocols might have the negative effects of increasing ED LOS and costs in overcrowded EDs. Further investigations concerning the overall effects of dedicated syncope units in the ED are needed.
Unfortunately, there was no significant reduction in major adverse events. This is one of our study's main limitations. We, however, focused on the efficacy of care provision in acute settings. In addition, to the best of our knowledge, most previous studies showed similar outcomes: that there were significant improvements in admission rates, medical costs and diagnostic yields without long-term data or with no significant differences in long-term outcomes.13,17,18,22
There are several other limitations to this study. First, this study was a nonrandomized, single center study. Also, we compared the two patient groups on a historical basis, and our sample size was too small for sufficient statistical power to assess all end points. Additionally, we could not evaluate whether or not our standardization procedure had any effect on morbidity and mortality. Therefore, our findings should be cautiously interpreted if considering similar implementation in other institutions. Second, we did not modify the diagnostic process outside the ED because our protocol was focused on ED evaluation. Hence, use of additional diagnostic tests was not strictly controlled. Further studies must be conducted after the adoption of a hospital-wide standardized protocol at our institution. Third, the approaches we used in our study might not be optimal and did not completely reflect the current guidelines, as we modified the guidelines to suit our hospital. For instance, basic blood tests and chest radiographs were conducted solely to prevent malpractice lawsuits, even when not clinically indicated. Fourth, we are unable to exclude the possibility that our findings resulted from a Hawthorne effect during the study period. Finally, we observed a difference in age between the two groups that might represent random variation or be associated with selection bias. However, we may have drawn the same conclusions after adjusting for potential confounders including age.
In conclusion, the implementation of standardized approaches to evaluate syncope reduced hospital admissions, medical costs and LOS in the overcrowded ED of a tertiary-care teaching hospital in South Korea.



 XML Download
XML Download