

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The management of thoracolumbar injuries has been a matter of debate, and the controversy is mostly related to the determination of fracture stability.1-4 Many classification schemes have been developed to guide clinical and surgical treatment of thoracolumbar injuries. We identified 4 thoracolumbar injury classification schemes that have been widely used and reported: the Denis classification,5 Magerl/AO classification,6 load sharing classification (LSC),7 and the thoracolumbar injury classification system (TLICS).8 These classification systems have been used implicitly to aid surgeons in deciding the best treatment option for individual patients.
Although easily reproduced and well accepted in many centers, the Denis system, which is based on the "three-column concept", is not detailed enough to account for all fracture types. In addition, it neither provides prognostic information nor accounts for the neurological status of patients, and therefore, it does not adequately guide surgical decision making. Although the Magerl classification, also known as the AO Spine system,5,6 accounted for some of these limitations by identifying a wide array of fractures, it does not account for the neurological status of patients, a critical determinant of surgical decision making.6
LSC, on the other hand, is a quantitative point system that has been proposed with a primarily therapeutic utility as a predictor of the failure of posterior short-segment fixation.7 Although it has not been extensively studied, 2 articles on LSC show a much better reproducibility for that classification than for either the Denis or AO systems.9,10 This is an interesting finding because LSC is basically a simple pattern recognition on diagnostic imaging.
TLICS, which is also a quantitative scoring system, identifies critical injury categories and assigns an injury severity score based on these categories that can guide spinal surgeons in surgical decision making with regard to thoracic or lumbar spinal trauma.8,11 This is the first classification system to specifically include the neurological status of the patient. More recently, the contribution of the posterior ligamentous complex (PLC) to spinal stability has become evident.8,12 PLC of the thoracolumbar spine is composed of the supraspinous and interspinous ligaments, ligamentum flavum, facet capsules, and thoracolumbar fascia. The recently proposed TLICS cites the integrity of PLC as one of the primary determinants of the need for surgical intervention.8
However, to our best knowledge, no report has elucidated the severity of damage of thoracic and lumbar burst fractures with classification schemes according to the presence of PLC injury. The aim of this study was to accurately assess the severity of damage in thoracic and lumbar burst fractures with PLC injuries and evaluate the relationship among the Denis classification, Magerl/AO classification, LSC, and TLICS according to the presence of PLC injury.
MATERIALS AND METHODS
A retrospective review was performed to identify treated adult patients with acute thoracic and/or lumbar burst fractures. One hundred consecutive patients (71 males and 29 females) were treated between April 1995 and December 2008 at a single institution. The mean age of the patients at the time of surgery was 36±17 years (range, 15-79 years). The exclusion criteria included major fractures at other sites, a significant associated injury to any other major organ system requiring hospital admission and active management, and pathological or osteoporotic delayed vertebral body collapse. After Institutional Review Board approval was given, each patient signed a written consent form before treatment.
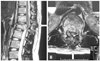
The diagnosis of thoracic and/or lumbar spinal trauma was established by plain radiographs, a computed tomography (CT) scan, and magnetic resonance imaging (MRI). These, in addition to the operation records, were then comprehensively reviewed by an experienced spinal surgeon participating in the study. These assessments were used to characterize the level of injury and the integrity of PLC at the involved spinal level. On preoperative plain radiographs and CT scans, this is typically indicated by splaying of the spinous processes (widening of the interspinous space), diastasis of the facet joints, and facet perch or subluxation.8 Other more indirect measures of posterior ligamentous disruption include vertebral body translation or rotation.8 In some cases, clinical examination may be helpful in determining the status of PLC. For example, a palpable gap between the spinous processes may show that PLC is disrupted.8 On preoperative MRI, in particular, PLC was characterized as either intact or disrupted. Intact PLC was defined as no visible change in the MRI signal, while disrupted PLC was defined as a clear MRI signal change with evidence of full discontinuity.13
Injury details, including the trauma etiology, were recorded. Injuries were also described as thoracic (T1-T10), thoracolumbar (T11-L2), or lumbar (L3-L5) spinal trauma. A neurological assessment was performed on each patient using a rating system, based on the American Spine Injury Association impairment scale (AIS). In addition, the fracture severity type was formulated according to the Denis and AO classifications, and the distributions of the fractures were similar. The totals of the severity scores were also evaluated according to LSC (Fig. 1: total 9 points) and TLICS (Table 1: total 10 points).
All patients were divided into 2 groups (the P group for those with PLC injuries and the C group for those without such injuries) for comparative study. The totals of the severity scores of LSC and TLICS were evaluated between the 2 groups. The ratio of patients who had an LSC score more than 7 points, suggesting anterior surgical treatment, was assessed. The ratio of patients who had a TLICS score more than 5 points, suggesting operative treatment, was also assessed. The TLICS score excluding the PLC score (total 7 points) was investigated between the 2 groups.
Statistical analysis
A standard StatView 5.0 software package (Abacus, Berkeley, CA, USA) was used for statistical analysis. All values are expressed as mean±standard deviation. An analysis of variance with a post hoc test (Mann-Whitney U test) was used for comparisons. The Spearman rank correlation coefficient was used to determine correlations. p<0.05 was considered statistically significant (Fig. 2).
RESULTS
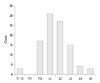
The causes of the fractures were as follows: fall from a height (77 patients), motor vehicle accident (11 patients), blunt contusion from the fall of a heavy object (8 patients), sledding accident (2 patients), and sports accident (2 patients). There were 3 patients with thoracic lesions (T6, T8, T10), 75 with thoracolumbar lesions (T11-L2), and 22 with lumbar lesions (L3-5) (Fig. 3). Preoperative AIS was A in 7, B in 6, C in 35, D in 28, and E in 24 patients. According to the Denis classification, Type A fracture was seen in 28, Type B in 48, Type C in 7, Type D in 10, and Type E in 7 patients. According to the AO classification, Type A fracture was seen in 59, Type B in 22, and Type C in 19 patients. The mean total score of TLICS was 6.4±2.7 points, while that of LSC was 7.2±1.4 points.
One hundred patients were divided into 2 groups that were included as part of a comparative examination: 41 patients (the P group; 22 males and 19 females) with PLC injuries and 59 patients (the C group; 50 males and 9 females) without such injuries, according to preoperative imaging studies. AIS was A in 6, B in 5, C in 15, D in 10, and E in 5 patients in the P group, and A in 1, B in 1, C in 20, D in 18, and E in 19 patients in the C group. Ninety percent of patients in the P group had neurological deficits, and AIS of the P group was more severe than that of the C group (Fig. 4). However, there was no potential for bias of the injured levels according to the presence of PLC injury. In the P group, according to the Denis classification, Type A fracture was seen in 11, Type B in 10, Type C in 3, Type D in 10, and Type E in 7 cases. In the C group, Type A was seen in 17, Type B in 38, and Type C in 4. The Denis Type D and E accounted for 41% of the P group (Fig. 5A). In the P group, according to the AO classification, Type B fracture was seen in 22 and Type C in 19 cases. Type A was seen in all patients of the C group (Fig. 5B).
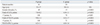
There were many women in P group in this study. Most of causes of their fractures were fall from a height by the suicide attempt. The LSC scores were significantly higher in the P group; 7.8±0.2 points for the P group and 6.9±1.1 points for the C group (p<0.001). All patients (100%) in the P group had an LSC score more than 7, suggesting anterior surgical treatment (Table 2). The total TLICS score was significantly higher in the P group; 9.0±1.3 points for the P group and 4.5±1.7 points for the C group (p<0.001). All 41 patients in the P group had a TLICS score of 5, or more. The TLICS score treatment recommendation for surgery agreed with the actual treatment provided in 100% of patients in the P group. The TLICS score (excluding the PLC score) was also significantly higher in the P group; 6.2±1.1 points for the P group and 4.0±1.4 points for the C group (p<0.001) (Table 2).
DISCUSSION
There is much controversy regarding thoracolumbar trauma diagnosis, treatment, and management. The present study reported the imaging evaluations of 100 patients with thoracic and lumbar burst fractures. The results showed that the damage in patients with PLC injuries was more severe than that in patients without such injuries in terms of the AIS, Denis, and AO classifications. The presence of PLC injury significantly influenced the severity of damage in terms of both LSC and TLICS, suggesting that TLICS can be used to classify thoracolumbar trauma and can accurately predict surgical management. In the management of thoracic and lumbar burst fractures, the evaluation of PLC injury is important to accurately assess the severity of damage.
The thoracolumbar region is the most commonly affected area in spinal trauma.14,15 The continuing effort to classify thoracolumbar spinal fractures reflects the contemporary difficulties encountered in defining or predicting the stability of such injuries. The diagnosis of presumed spinal instability following trauma has traditionally been based on an assessment of MRI, and biomechanical engineers and clinicians have been constrained to the use of such diagnostic tools as routine plain radiographs, CT scans, and MRIs in developing a universally accepted definition of stability.8 White and Panjabi16,17 devised the most comprehensive definition: "Clinical instability is defined as a loss in the ability of the spine under physiological loads to maintain relationships between vertebrae in such a way that there is neither damage nor subsequent irritation to the spinal cord or nerve roots. In addition, there is no development of incapacitating deformity or pain due to structural changes". Decisions regarding the treatment of thoracolumbar injuries often hinge on the presence or absence of spinal stability, although it is not always easy to determine the stability of the involved spinal segments.
LSC has been proposed primarily with a therapeutic utility as a predictor of the failure of posterior short-segment fixation.7 This is an interesting finding because LSC is basically consisted of simple pattern recognition on diagnostic imaging. LSC could be used for guiding the treatment of thoracolumbar burst fractures not only in surgical approach choice, but also surgical decision making.18
The Spine Trauma Study Group recently described a classification system for thoracolumbar injury that is referred to as TLICS.8 TLICS incorporates clinically important injury characteristics that are then used to aid in surgical decision-making. Within this classification system, there are 3 "primary axes" that are independently important and complementary to one another in the characterization and treatment of fracture patterns: 1) injury morphology, 2) integrity of PLC, and 3) neurological status. A severity score is used in conjunction with the classification system to help guide the treatment decision-making process.12 This classification system has been shown in numerous studies to be both valid and reproducible.19-21 Appropriate use of TLICS requires reliable assessment of the integrity of PLC.18
The contribution of PLC to spinal stability has become evident. The recently proposed TLICS for thoracolumbar injury cites the integrity of PLC as one of the primary determinants of the need for surgical intervention.8 Complete disruption of PLC, as determined collectively by morphological criteria based on imaging studies, is an indication for surgical intervention in thoracolumbar burst fractures.12 The LSC and TLICS scores accurately reflect the severity of the injury. The inclusion of this critical clinical variable likely accounts for the high rate of agreement between the TLICS score and historical surgical cohorts.20 TLICS and severity scores are easily applied and have been shown to match prior surgical indications while having the advantage of being able to systematize those indications. Moreover, they can give the treating physician an idea of the injury severity, given the relationship between the TLICS score and worse spinal cord injury. This suggests that TLICS can be used to classify thoracic and lumbar trauma and can accurately detect the severity of damage.
This study had several limitations. Although a retrospective review was performed to identify patients treated surgically for thoracolumbar spine injuries, clinical and radiographic reviewers were blinded to the ultimate treatment results. This did not add potential bias to the use and calculation of the LSC and TLICS scores.
In conclusion, the presence of PLC injury significantly influenced the severity of damage. In the management of thoracic and lumbar burst fractures, the evaluation of PLC injury is important to accurately assess the severity of damage.




 XML Download
XML Download