

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Glioblastoma (GBM) is the most common primary malignant brain tumor in adults. Due to its diffuse infiltrative growth, radical resection is usually impossible and most recurrences occur in the vicinity of original sites.1 Ever since postoperative radiotherapy was introduced survival has improved;2,3 however, the prognosis of GBM is remains poor with a median survival of around one year. The addition of temozolomide to radiotherapy has enhanced survival, but only by about 2-3 months.4,5 These poor prognoses highlight the need for new effective therapeutic approaches, in addition to current treatments, to improve survival outcomes.
In contrast to normal cells, whose growth is regulated by organized growth stimulatory pathways, the growth of cancer cells is dysregulated and activated constitutively by multiple pathways. Epidermal growth factor receptor (EGFR) plays a central role in both development and tumorigenesis within many organ systems, including the central nervous system.6 The EGFR gene is the most commonly amplified gene in GBMs and is amplified several times in tumor cells, compared to normal cells.7-9 Overexpression of EGFR appears to correlate with glioma grade, which is observed in about 40-50% of GBMs, compared to 10-26% of anaplastic astrocytomas.10,11 Therefore, EGFR may potentially be a grading markers of GBMs.
Among researchers the prognostic significance of EGFR expression in GBM patients is still debated. Some have found poor prognoses to be associated with amplification of the EGFR gene or overexpression of EGFR in GBM patients,12-17 while others have not.11,18-24 Therefore, we conducted this retrospective analysis to evaluate the impact of EGFR expression on the clinical outcomes of GBM patients who received surgery and postoperative radiotherapy at a single institution in order to obviate treatment related biases as much as possible.
MATERIALS AND METHODS
Patients
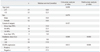
Thirty three consecutive GBM patients who had received both surgery and postoperative radiotherapy at our institution, between March 1997 and February 2006, were reviewed. As tissue specimens were lost for three patients, only 30 patients were finally included in the analysis. Analysis of these patients was approved by the Institutional Review Board. Patients were followed until their death, with four patients still living at the time of the analysis. All patients received conventional radiotherapy, 1.8-2.0 Gy/day, for about 4-6 weeks after operation. Three patients received less than 50 Gy because of tumor progression at 44.0 Gy, sepsis attributed to aspiration pneumonia at 12.6 Gy, and refusal of further radiotherapy at 37.8 Gy. Excluding these, the remaining 27 patients received doses of 50 Gy or greater (median: 61.2 Gy, range: 55.2-65.1 Gy). Median age at diagnosis was 55.5 years (range: 24-77 years). There were 18 male and 12 female patients. Resection of at least 50% of tumor was done in 20 patients, less than 50% tumor resection in eight, and biopsy in two patients (Table 1).
Immunohistochemical staining
Formalin-fixed and paraffin embedded tissue blocks were cut serially into 4 µm thick sections. All processes of immunohistochemistry were performed automatically using a Ventana autostainer (Benchmark; Ventana Medical Systems, Tucson, AZ, USA). For antigen retrieval, retrieval solution (Ventana) was automatically poured on the sections, and then the sections were heated at 100℃ for 60 minutes. Endogenous peroxide activity was blocked by immersion in 3% hydrogen peroxide for four minutes. With primary antibodies for EGFR (mouse monoclonal antibody, 1 : 1, Zymed; Invitrogen, Camarillo, CA, USA), the tissue sections were incubated for 32 minutes at 36℃. Immunoperoxidase staining was performed with the DAB system (iView DAB detection kit; Ventana Medical Systems, Tucson, AZ, USA), and then the sections were lightly counterstained with hematoxylin.
Evaluation of EGFR expression
Two pathologists independently interpreted the results of immunohistochemical studies without any clinical or other histological information. Intensity of staining was assessed gradually (0, negative; 1, weak; 2, intermediate; 3, strong), and a grade of more than two (intermediate or strong intensity) was considered representative of positive cells. The percentage of positive cells in a tumor mass was measured by the pathologists. Immunohistochemical staining was considered positive when more than 10% of tumor cells showed membranous or cytoplasmic immunoreactivity.
Statistical analysis
Fisher's exact test was used for the evaluation of the associations between EGFR expression and patient characteristics. Survival was measured from the date of the surgery for GBM. Survival analysis was carried out with the Kaplan-Meier method and a log rank test. Multivariate analysis was performed with a Cox proportional hazards model. Statistical analyses were performed using SPSS software version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
EGFR immunostaining
The expression of EGFR was positive in 23 patients among the 30 patients whose specimens were available for study (Table 1). EGFR expression was predominately located in the cell membrane of the GBM, followed by that in the cytoplasm (Fig. 1). Expression in the nuclear membrane was found in three patients. EGFR was strongly stained in all positive specimens, negating the need to perform analysis of intensity differences among positive slides. Instead, the percentage of EGFR positive cells out of all tumor cells was counted. EGFR expression was not different according to patient characteristics, such as age, sex, extent of surgical resection, and radiation dose (Table 2).
Clinical factors and survival
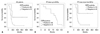
The median survival was 13.0 months, and 1- and 2-year survival rates were 63.3% and 16.7%, respectively. On univariate analysis, a higher radiation dose (>60 Gy vs. ≤60 Gy) and negative EGFR expression (negative vs. positive) were significantly correlated with improved survival, the median survivals of which were 17.0 months vs. 9.0 months (p=0.000) and 17.5 months vs. 12.5 months (p=0.013), respectively. After multivariate analysis, a higher radiation dose and negative EGFR expression remained significant in their association with improved survival (Table 3) (Fig. 2). Although the small patient number in each group may make the statistical difference thereof be of little importance, negative EGFR expression was significantly correlated with better survival in the patient groups of >60 Gy and ≤60 Gy (p=0.037 and p=0.020, respectively). There were four long-term survivors who were alive at the time of the analysis. The percentages of EGFR expressing cells in their specimens were at most 5%; three were 0% and one was 5%.
DISCUSSION
Although EGFR is the most commonly amplified gene in GBM patients, the prognostic significance of EGFR has remained controversial. EGFR expression can be examined at the gene, DNA, RNA, and protein level. To do so, immunohistochemistry has been widely used for the evaluation of EGFR expression on paraffin-embedded tumor specimens. However, the determination of EGFR immunoreactivity could be affected by multiple factors, such as the choice of fixative, the storage time of tumor tissue, the choice of antibody, and the lack of criteria for evaluation.25-28 Therefore, a method that is less dependent on the above factors should be developed.
The present study used immunohistochemical staining for the analysis of EGFR expression in GBM tissues. In the literature, results for the influence of EGFR expression on survival according to immunohistochemical staining differed among researchers (Table 4). Some insisted that EGFR expression had a negative effect on survival compared to non-expression.16,17 Others argued that EGFR expression had an insignificant effect on survival.19,20 The median survival of patients exhibiting EGFR expressing GBM cells was significantly less than that of EGFR negative patients in the present study.
The definition of EGFR positivity can be influenced by stain intensity and the fraction of stained cells. Because the intensity of EGFR expression was homogenously strong in all positive specimens of this study, guidelines for positivity could be drawn according to the percentage of positive cells without consideration of any staining intensity. In addition to the initial EGFR positivity, based on the presence of any positive cells, several cutoff points were taken into consideration for further analysis (Table 5). When 10% and 20% positive cells among GBM cells were used as the lowest cutoff points for EGFR positivity, the survival rates of EGFR positive patients were significantly lower than that of EGFR negative patients. Moreover, survival was not different when the lowest cutoff point of 30% was applied.
Analyzing Radiation Therapy Oncology Group (RTOG) trial data, Chakravarti, et al.18 showed that immunohistochemically determined total EGFR levels were not of prognostic value in GBM patients. They selected 155 GBM patients from the RTOG trials of 7401, 7918, 8302, 8409, 9006, 9305, 9602, and 9806. However, the radiotherapy methods applied in the trials were heterogenous. Irradiation volume ranged from peritumoral to the whole brain, in addition to varying radiation doses from 48 Gy to 81.6 Gy, and fractionation schemes from conventional, hyperfraction, to stereotactic radiosurgery boost. Therefore, in order to obtain a reliable conclusion, it was necessary to conduct an EGFR study with data from more homogenously managed patients. Patients in the present study were treated at a single hospital, so they were considered to have been managed similarly. The present study observed significantly poorer outcomes in EGFR expressing patients; however, these results were observed in only a small number of patients, which may make the results less valuable.
Because most recurrences in GBM patients occur within two cm of the pre-surgical, initial tumor margin,1 delivering a larger dose to improve local control and survival is necessary. However, confirmatory data to support that irradiation of more than 60 Gy improves prognoses in GBM patients is lacking.29,30 Recently, RTOG conducted a radiation dose escalation study using three dimensional conformal radiotherapy (3DCRT), and found that delivering a higher than standard (60 Gy) radiotherapy dose was feasible with an acceptable risk of late central nervous system toxicity.31 This study applied 3DCRT in all patients, and the patients that received greater than 60 Gy demonstrated better survival than those irradiated with 60 Gy or less. The survival conbenefit of patients receiving higher than 60 Gy was sustained after excluding less than 50 Gy (data not shown) in the analysis. Therefore, radiation dose escalation trials should be tried with sophisticated radiotherapy methods, such as 3DCRT, intensity modulated radiotherapy, stereotactic radiotherapy, radiosurgery, and proton therapy.
The effect of surgical resection extent in the treatment of GBM is still under debate,32-35 but an inferior survival in patients who undergo biopsy only compared to surgery was evident in most studies.32,36,37 We also found that survival was lower in patients that underwent less than 10% resection compared to patients who underwent greater surgical resection, although the difference was not significant (Table 3). Moreover, there were only two patients with less than 10% resection in this study, so further analysis with more patients may provide more statistically powerful results.
To obtain more confirmatory or less biased results of EGFR expression on survival in GBM patients, data from a large number of GBM patients who were treated homogenously are needed. When the prognostic significance of EGFR expression is verified, we should have another option for which to treat GBM patients, in addition to the unsatisfactory treatment modalities currently available.





 XML Download
XML Download