

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Renal cell carcinoma (RCC) occupies 3% of adult cancers and 22% of urologic cancers in Korea, and the development of diagnostic tools had lead to increases in the incidental detection rate of localized small RCC.1
Prognostic factors in small RCC include TNM stage at diagnosis, presence of symptoms, tumor size, and nuclear grade.2-4 Pathologic stage is known to be the most accurate prognostic factor in RCC,5,6 and T stage is considered the most important factor affecting survival in the non-metastatic RCC.1
Urologists often encounter T1 tumors on preoperative imaging study that are revealed to be T3a (perirenal fat infiltration only) on pathologic report. Moreover, there is debate as to whether perirenal fat infiltration is associated with prognoses of RCC.
Siemer, et al.7 suggested that perirenal fat infiltration is not a prognostic predictor of cancer specific survival, and pT3a tumors of 7 cm or less should be included in stage T1. Gofrit, et al.8 also suggested that perirenal fat infiltration should be removed from the current TNM staging system because T3a stage includes a heterogenous group of disease.
We evaluated whether the presence of perirenal fat infiltration can be a prognostic factor in these small RCCs.
MATERIALS AND METHODS
Of 365 patients who underwent radical nephrectomy for RCC at our institution between 1994 and 2006, we retrospectively reviewed the medical records of 164 cases of tumors 7 cm or less in size. Patients with bilateral RCC, RCC related to von Hippel-Lindau disease or end stage renal disease, or RCC with adrenal gland, lymph node invasion or distant metastasis, were excluded.
Following surgery, all patients were evaluated with physical examination, serum laboratory studies and radiologic studies including computed tomography for local recurrence or distant metastasis every 3 months for first 1 year, every 6 months for next 2 years, and yearly thereafter.
Pathological staging was performed with the 2002 TNM classification9 and histological subtyping was performed by the 2004 WHO classification.10 Each tumor was graded according to the Fuhrman nuclear grading system.11
We divided the patients into two groups according to the presence of perirenal fat infiltration (group A, pT1; group B, pT3a). We evaluated the relationships, recurrence-free survival and disease-specific survival according to age, sex, cell type, nuclear grade, presence of sarcomatoid component and coagulative histologic necrosis. Overall survival was estimated using Kaplan-Meyer method and statistical differences in survival between the groups were calculated by the log-rank test. Multivariate analysis using Cox proportional hazard model was performed to investigate factors for predicting recurrence-free survival.
RESULTS
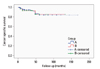
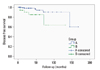
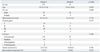
A total 131 patients were included in group A (pT1), with a mean age of 55.8 (±11.6) years, an average tumor size of 4.2 (±1.4) cm, and a mean follow-up period of 43 months. Group B (pT3a) included 33 patients, with a mean age of 55.9 (±10.6) years, an average tumor size of 4.1 (±1.6) cm, and a mean follow-up period of 38 months. No significant difference in patient demographics was noted between the two groups. In the comparison between two groups, in regards to prognostic factors, no significant difference was discovered (Table 1). There was also no significant difference in estimated disease-specific survival between the two groups (p=0.90) (Fig. 1); however, recurrence-free survival was significantly different between the two groups (group A: 95.5%, group B: 84.4%, p=0.009) (Fig. 2).
DISCUSSION
In a recent report, the detection rate of locally confined RCC was shown to be increasing1 consequently allowing for greater chances to treat small (T1) cancers.
T1 tumors diagnosed by preoperative imaging study exhibiting perienal fat infiltration on pathologic results is reported up to 31%, and several opinions have been offered for whether this upstaging of the disease affects the prognosis.12-16 Lapini, et al.13 and Puppo, et al.16 reported that upstaging of the disease led to higher metastasis rates and poorer prognoses. Han, et al.17 reported similar results; however, Roberts, et al.12 reported no difference in 5-year survival rate between a pT1 group and pT3a group, unless presented with tumor invasion of surgical resection margins.
Robson, et al.18 first suggested that cases of perirenal infiltration of tumors showed poorer survival rate than those of cases confined to the kidney. Patard, et al. reported that perirenal fat infiltration is indeed an independent prognostic factor.19
According to the current TNM 2002 staging, perirenal fat, sinus fat and/or adrenal gland involvement are all classified as T3a.9 However, the prognostic value of perirenal fat infiltration has not yet to be universally accepted. Some reports noted that disease-free survival and cancer specific survival for pT3a renal cell carcinoma was equivalent or better than that in pT1 or pT2 tumors.20-22
In localized RCC, tumor size is accepted as a factor for predicting patient's prognosis, and some authors have suggested that a cut-off of 7 cm in size in T1 disease is too inclusive and more subdivided cut-off value is necessary to better predict progroses.15 However, Minervini, et al.23 noted that the 7 cm cut-off better demonstrated a significant difference in survival, so that the TNM classification, revised in 1977, accepted 7 cm as a cut-off for dividing T1 and T2 tumors. Accordingly, we applied 7 cm as a criterion for defining "small" cancers in this study.
Recent studies showed that the size of a tumor is an important prognostic factor in pT3a RCC with perirenal fat infiltration only, suggesting that tumor size and perirenal fat infiltration should be included in T3a RCC staging.24,25 Yoo, et al.25 noted that pT3a RCC of 7 cm or less exhibited poorer disease-free survival, but showed similar cancer specific survival with pT1 RCC. Perirenal fat infiltration was an independent prognostic factor for disease-free survival but not for cancer specific survival. Additionally, Jeon, et al.26 reported that perirenal fat infiltration was prognostically significant in tumors greater than 7 cm but not in those of 7 cm or less.
As the importance of perirenal fat infiltration as a criterion in pT3a is doubted, some authors suggest that T3a stage should be revised. In our results, perirenal fat infiltration was an independent prognostic factor in small (<7 cm) RCC. Although no significant difference in disease-specific survival was noted, recurrence-free survival did show a significant difference. Although these results are inconsistent with the results of earlier studies,25,26 all of these studies, including ours, were retrospectively investigated and did not include a large enough sample size. Accordingly larger scaled prospective multicenter study may yield results that are more consistent.
TNM stage at diagnosis, presence of symptoms, tumor size, nuclear grade, etc. are known as prognostic factors in localized (pT1) RCC.2-4 However, few data is available for significant prognostic factors in small (<7 cm) RCCs with perirenal fat infiltration. In our study, nuclear grade was the only significant factor predictive of disease-free survival in the presence of perirenal fat infiltration.
We propose that even in case of preoperatively T1 RCC, if the perirenal fat infiltration is present on postoperative histopathologic reports, especially in those of high nuclear grade, clinicians should follow-up the patients more strictly.
The retrospective nature of our study, as well as the sample size, limits the interpretation of our results. However, further prospective studies may confirm the importance of the presence of perirenal fat infiltration in RCC. In conclusion, the presence of perirenal fat infiltration was an independent prognostic factor for predicting disease-free survival in patients who underwent surgery for small (<7 cm) renal cell carcinoma. Therefore, as this study showed, the presence of perirenal fat infiltration requires stricter follow-up planning, even in small renal cell carcinoma.
 XML Download
XML Download