

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since Bentall and De Bono1 first described composite valve graft implantation in 1968, this well documented technique of aortic root replacement has been used for a large spectrum of various pathologic conditions involving the aortic valve, aortic root, and ascending aorta.2-4 In this study, we retrospectively reviewed and evaluated the early and long-term results of our 28-year clinical experience with the Bentall procedure for various aortic diseases in 218 patients.
MATERIALS AND METHODS
Patients' characteristics
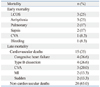
From March 1982 to December 2010, a total of 218 patients underwent the Bentall procedure using a composite valved conduit in Yonsei Cardiovascular Center, Yonsei University Health System. Our study was conducted with the approval of the Institutional Review Board of Yonsei University College of Medicine (Yonsei Institutional Review Board No. 4-2011-0062). Individual patient consent was waived. The mean patient age at the time of the operation was 44.4±13.9 years (range, 13-76 years). Of these patients, 151 (69%) were male and 67 were female (31%). The preoperative diagnoses included annuloaortic ectasia (144), acute aortic dissection (DeBakey type I: 29, type II: 9), chronic aortic dissection (type I: 12, type II: 18), and annular endocarditis (9). The causes of aortic disease included Marfan syndrome in 102 patients (46.8%), atherosclerosis in 64 patients (29.4%), congenital bicuspid aortic valve in 39 patients (17.9%), bacterial endocarditis in 9 patients (4.1%), syphilitic aortitis in 3 patients (1.4%), and Takayasu arteritis in one patient (0.5%). Twenty patients (9.8%) had previously undergone surgical intervention on the aortic valve or ascending aorta, or both. Nine patients (4.1%) were in New York Heart Association (NYHA) functional class I, 92 patients (42.2%) in class II, 89 patients (40.8%) in class III, and 28 patients (12.8%) in class IV (Table 1).
Surgical techniques
The operation was performed through a standard median sternotomy, and cardiopulmonary bypass was instituted by cannulation of the ascending aorta, aortic arch, femoral artery, or subclavian artery, and the right atrium. Myocardial protection was achieved by antegrade, retrograde, or simultaneously antegrade and retrograde intermittent cold hyperkalemic blood cardioplegia. The "inclusion technique" was performed in 30 patients (13.8%), the "open-button technique" in 181 patients (83.0%), and the Cabrol technique in 7 patients (3.2%). In patients treated with "open-button technique", coronary reimplantation suture lines were reinforced with an autologous pericardial strip or removed aortic wall. The Cabrol technique was used only in cases of reoperation because of difficulty with mobilizing and approximating coronary arteries to the vascular graft.
The concomitant procedures included graft replacement of the ascending aorta (9); hemi arch (11), total arch (7), or mitral valve replacement (4); mitral annuloplasty (14), coronary artery bypass grafting (21); repair of a ventricular septal defect (4); tricuspid valve repair (10); myectomy (2); and the Dor procedure (1). In cases of arch or hemi arch replacement, cerebral protection was obtained with deep hypothermic circulatory arrest (DHCA) in 3 patients, DHCA and retrograde cerebral perfusion in 8 patients, and antegrade cerebral perfusion through the right subclavian artery with moderate systemic hypothermia in 7 patients.
A Bjork-Shiley composite graft prosthesis (Shiley, Inc., Irvine, CA, USA) was used in 11 patients; a St. Jude composite graft (St. Jude Medical, Inc., St. Paul, MN, USA) in 146 patients; a Carbomedics composite graft (Carbomedics, Inc., Austin, TX, USA) in 52 patients; ATS (ATS Medical, Inc., Minneapolis, MN, USA) in 1 patient; freestyle stentless valve (Medtronic, Inc., Minneapolis, MN, USA) in 5 patients; and aortic homograft in 3 patients (Table 2).
Follow-up and statistical analysis
All patients were followed in the outpatient department with clinical examination, computed tomography scans and transthoracic echocardiography. When necessary, patients were interviewed via the telephone to obtain actualized information. Among 206 hospital survivors, 196 (95.1%) patients were available for follow-up (mean: 108 months). Statistical analysis was performed with the SPSS 11.0 statistical software package (SPSS, Chicago, IL, USA). Continuous variables were expressed as the mean±standard deviation, and compared with unpaired two-tailed t-test. Categorical variables were analyzed with the χ2 test or Fisher's exact test, where appropriate. Univariate and multivariate analysis of predictors for early and late mortality were performed using a logistic regression model. A p-value of <0.05 was considered statistically significant. Survival curves were constructed using the Kaplan-Meier method and compared with the log-rank test.
RESULTS
Hospital mortality and morbidity
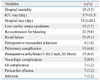
The overall early mortality rate, defined as death within 30 days of initial hospitalization, was 5.5% (12/218). Causes of death were low cardiac output syndrome in 3, ventricular arrhythmia in 3, pneumonia or acute respiratory distress syndrome in 2, sepsis in 2, cerebrovascular accident in 1, and bleeding in 1 patient (Table 3). Early complications included re-exploration for bleeding in 21, acute renal failure in 20, low cardiac output syndrome in 12, upper gastrointestinal bleeding in 7, myocardial infarction in 4, prolonged mechanical ventilation in 10, pericardial effusion in 7, transient ischemic attack in 1, cerebral infarction in 1, and superficial wound infection in 7 patients (Table 4A).
Postoperative left ventricular end-systolic dimension significantly decreased from 50.9±12.4 to 43.1±11.4 mm (p<0.001), and left ventricular end-diastolic dimension significantly decreased from 69.2±12.4 to 57.3±11.1 mm (p<0.001). The postoperative NYHA functional class also improved significantly (2.59±0.76 to 1.14±0.39, p<0.001), and ascending aortic size measured with pre and postoperative chest computed tomography (CT) decreased from 70.0±19.9 to 32.4±4.4 mm (p<0.001).
In hospital mortality was significantly affected by preoperative diabetes mellitus [odds ratio (OR) 16.62; 95% confidence interval (CI) 2.58 to 106.91; p=0.003] and NYHA class of 3 or greater (OR 5.28; 95% CI, 1.06 to 26.10; p=0.041) (Table 5).
Late mortality and survival
The mean follow-up duration was 108.0±81.0 months (range: 1-329 months). During the follow-up period, 15 cardiac-related (6.9%) and 28 non-cardiac-related (12.8%) deaths occurred. The most common causes of cardiac-related death were congestive heart failure (n=4) and type B dissection progression (n=4). The causes of cardiac-related late death are listed in Table 3.
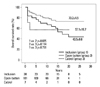
Kaplan-Meier estimated overall survival rates for the 218 patients (including hospital deaths) were 90.4±2.0%, 82.7±2.7%, 77.6±3.1%, 65.3±4.6%, and 60.3±6.4% at 1, 5, 10, 20, and 25 years, respectively (Fig. 1A). Among the patients with Marfan syndrome, the overall survival rate tended to decline compared to the group without Marfan syndrome, but did not reach statistical significance (log rank p=0.586) (Fig. 1B). Among the patients with dissection, the overall survival rate was not different compared to the group without dissection (log rank p=0.550) (Fig. 2A). However, among patients with acute dissection, the overall survival rate was significantly lower than that of the group with chronic dissection (Fig. 2B). Overall survival rates between the non-dissection group and the chronic dissection group were similar. Among patients treated with the open-button technique, the overall survival rate was better than that for those treated with the inclusion technique or Cabrol technique (Fig. 3). Univariate analyses revealed that hypertension, chronic renal failure, NYHA class of 3 or greater, and coronary transfer technique were risk factors for late death. Multivariate logistic analysis identified hypertension as the only independent risk factor for late death (OR 2.51, 95% CI, 1.14 to 5.53; p=0.022) (Table 5).
Late morbidity
Late complications included new onset aneurysm or dissection in 13, intracranial hemorrhage in 3, cerebral infarction in 6, gastrointestinal bleeding in 3, pericardial effusion requiring pericardiocentesis in 5, arrhythmia in 4, and bacterial endocarditis in 3 patients (Table 4B).
Reoperation
One patient who underwent the Bentall operation with a homograft required a redo Bentall operation due to homograft dehiscence and residual moderate aortic regurgitation. One patient required reoperation for development of a coronary pseudoaneurysm 20 years after a Bentall procedure had been performed using the inclusion technique. Seven patients required re-operation for progression of aortic arch, descending thoracic aortic dissection or aneurysm within a mean of 100 months (range: 1-204 months) after the first operation. Four of these patients had Marfan syndrome. One patient required stent graft insertion for descending thoracic aortic dissection, and he also had Marfan syndrome. The Kaplan-Meier analysis for freedom from reoperation is shown in Fig. 2. Freedom from re-operation rates for all patients at 1, 5, 10, 20, and 25 years were 99.0±0.7%, 98.3± 1.0%, 95.5±1.7%, 90.8±3.9%, and 90.8±3.9%, respectively (Fig. 4A). In patients with Marfan syndrome, survival without reoperation tended to decline compared to the group without Marfan syndrome, but this observation did not reach statistical significance (log rank p=0.089) (Fig. 4B).
Freedom from prosthetic valve-related complications
During the follow-up period, nine anticoagulant-related complications occurred. Cerebral hemorrhage occurred in 4 patients, two of which died from cerebral hemorrhage. Gastrointestinal bleeding occurred in 4 patients and coumadin toxicity occurred in 1 patient. All of these patients were treated with medical therapy and recovered. Freedom from anticoagulant-related complications was 95.9±1.1%, 94.2±1.7% and 92.9±0.2% at 5, 10 and 25 years, respectively (Fig. 5A). After discharge, 3 patients experienced prosthetic valve endocarditis. Two of these patients healed after medical therapy, while the other patient died from rupture of an intracranial mycotic aneurysm. Freedom from prosthetic valve endocarditis rate was 99.0±0.7%, 97.1±2.0% and 97.1±2.0% at 5, 10, and 25 years, respectively (Fig. 5B). Freedom from prosthetic valve related complications was 98.1±1.0%, 93.3±1.9%, 92.4±2.1% and 89.3±3.0% at 1, 5, 10, and 25 years, respectively (Fig. 5C).
DISCUSSION
The original Bentall procedure has been widely used since 1968 when Bentall and De Bono1 first described the technique. Over the past decades, several modifications of the originally described technique have been introduced, and have helped to improve clinical outcomes.2-5
Although results, following introduction of the Bentall procedure, have steadily improved, over the last decade, various kinds of valve-sparing operations have become an attractive alternative to replacement of the aortic root, improving survival with fewer complications and better quality of life, even in patients with Marfan syndrome.6-9 However, due to the complexity of the procedure it is still regarded as a challenging procedure, especially in emergency settings, e.g. cases of acute aortic dissection, and if the damaged aortic valve is combined with dilatation of the aortic root or a dissection, the Bentall procedure is required. It is also remains questionable as to whether a valve-sparing procedure is suitable only for specific patients or is more widely applicable, and whether the long-term durability is better than that of replacement. Therefore, the modified Bentall procedure is likely to remain the standard approach for various aortic root diseases.
When Bentall and De Bono1 first performed this procedure, a star valve was sutured into a tube graft to form a composite graft. Since then, mechanical vales have been generally used. The grafts often used for the Bentall procedure are composite grafts, cryo-preserved homografts, autologous pulmonary valves, and stentless valves. Since the availability of cryo-preserved homografts is limited, we use homografts only in patients with active infective endocarditis. The decision whether to use a mechanical or biologic valve was made on an individual basis by the surgeon and the patient. Even though mechanical valves were used in most patients, the rates of valve-related complications seemed to be similar to that of sole aortic valve replacement, as previously described by other authors.10
One of the most important portions of the Bentall procedure is the coronary anastomosis technique. Three different anastomotic techniques have been developed over the past few decades: the inclusion, button, and Cabrol techniques. The inclusion technique, as originally described by Bentall and De Bono1 was until 1993 our preferred method. Many authors had reported a relationship between the inclusion/wrapping technique, and the formation of coronary pseudoaneurysm, especially in patients with Marfan syndrome.11-14 The incidence of pseudoaneurysms with this technique ranged from 7% to 25%.15-17 However, since aortography or aorta CT is not performed on all patients after the Bentall procedure, the true frequency may have been higher. Our experience also showed that the open-button technique was better than the inclusion technique in regards to long-term survival (Fig. 3). Although we have not experienced pseudoaneurysm during the earlier period, we had one patient who was re-operated for coronary pseudoaneurysm 20 years after undergoing the Bentall procedure using the inclusion technique. Since a long interval between the operation and the development of pseudoaneurysm is not unusual, continuous careful follow-up of patients with imaging studies is suggested. We abandoned performing the inclusion technique in 1994, and the open button technique in its stead, which includes direct implantation of coronary buttons and a distal anastomosis to the completely divided ascending aorta, has remained the current policy for aortic root replacement at our institute. We also adopted a technique of preclotting the prosthesis with albumin plus autoclaving in 1994, which further contributed to reoperation rate decline. The Cabrol technique was used only in cases of re-operation because of difficulties with mobilization and approximation of coronary arteries to the vascular graft or upon extensive calcification of the aneurismal aorta.
Numerous studies have shown different independent risk factors for death after the Bentall procedure.18,19 Advanced age, dissection, Marfan syndrome, severe ventricular dysfunction, endocarditis, previous cardiac surgery, emergency status, coronary artery disease, poor preoperative New York Heart Association functional class and left ventricle ejection fraction <35% were known as predictors of early and late death. We observed that hospital mortality was strongly correlated with diabetes mellitus and NYHA class (≥3), and late death was strongly correlated with hypertension. We believe that diabetes mellitus and a NYHA functional class associated with early morbidity seem to be correlated with hospital mortality. Hypertension seems to be an independent risk factor of late death in regard that common reasons of late death included congestive heart failure, type B dissection progression, and cerebral vascular accident, which are all associated with hypertension. With improvements in operative technique and postoperative management, advanced age, dissection, Marfan syndrome, endocarditis, and previous cardiac surgery did not prove to be independent risk factors for early mortality in this study. We did experience different results, however, between acute dissection and chronic dissection (Fig. 2B). This showed that acute dissection was still risk factor of after Bentall procedure.
There are many debates as to whether Marfan syndrome is associated with long-term survival or not, after the Bentall procedure. Yousif and colleagues reported that Marfan was an independent risk factor of long-term mortality.20 However, Hagl, et al.5 demonstrated that Marfan syndrome was not associated with lower long-term survival. In our study, although there was a trend for decreased survival of patients with Marfan syndrome in the course of time compared to that of non-Marfan patients (Fig. 1B), we could not find a significant association for Marfan syndrome with long-term survival (p=0.586). However, we found that Marfan syndrome was strongly associated with the incidence of reoperation during follow-up. Many authors have reported a high incidence of subsequent operations on the remaining aorta in patients with Marfan syndrome. Kouchoukos, et al.2 reported that at 12 years, the actual probability of freedom from re-operation was significantly lower in patients with Marfan syndrome (85%), compared to patients without Marfan syndrome (96%). A similarly high incidence rate of re-operation on the remaining aorta in Marfan patients was reported by Crawford.21 In our study, among seven patients who required re-operation, 4 patients had Marfan syndrome. One patient who required stent graft insertion for descending thoracic dissection also had Marfan syndrome. These facts imply that these patients require careful medication to strictly control blood pressure and heart rate, as well as periodic evaluation of the entire aorta throughout their life.
Early mortality after the Bentall procedure was reported to range from 1.9% to 7.3%.22,23 Although there may be some differences therefore according to the type of patient undergoing the operation (percentage of acute aortic dissection, or Marfan patients, for instance), most authors report low hospital mortality, as well as a significant difference between patients receiving emergency surgery versus receiving elective surgery.23 In our study, the operative mortality rate was 5.5% which was comparable to other studies. Functional status improved in most patients with good long-term outcomes.
Prosthetic valve-related complications in our study were also comparable to other reports. Freedom from anticoagulation-related complications at 25 years was 93%. Prosthetic endocarditis occurred only in 3 (1.3%) of the followed patients, which was significantly lower than previously reported incidences.
In summary, we have found that, in our experience, operative mortality and long-term survival after the Bentall procedure were comparable to that in other studies, and open-button Bentall operation can be performed with excellent short-term and long-term results. However, re-operation of the remaining aorta is not rare especially in the Marfan population; therefore, continuous follow-up and proper medical management is recommended.








 XML Download
XML Download