

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Inflammatory reactions occur early after coronary stent implantation and play an important role in the pathogenesis of neointimal hyperplasia.1 After stenting, T cells, macrophages, and smooth muscle cells are recruited to the implantation site; and this local inflammatory response is thought to correlate with restenosis.2 Cyclooxygenase (COX) is the principal enzyme involved in the production of prostaglandins, which are induced by tissue injury and implicated in the inflammatory response.3 The COX-2 isoenzyme is expressed in macrophages, smooth muscle, and endothelial cells of human atherosclerotic plaques, and is thought to promote neointimal growth after stent implantation.4 Matrix metalloproteinase (MMP) is an another important enzyme that has been implicated in the pathogenesis of restenosis. The activation of MMP has been shown to contribute to neointimal hyperplasia after vascular injury by controlling extracellular matrix degradation and facilitating intimal remodeling.5,6 Although results of animal studies are conflicting,7-9 a recent clinical trial showed that prolonged inhibition of COX-2 with celecoxib was effective in reducing restenosis.10 However, concerns about the safety of COX-2 inhibitors in terms of increased thrombosis and elevated blood pressure remain,11,12 and long-term use of COX-2 inhibitors in patients with cardiovascular disease is still not generally favored. Doxycycline, a derivative of tetracycline, is a nonspecific MMP inhibitor that has been shown to reduce neointimal hyperplasia in animal models.13 However, no clinical trials have been carried out on the effect of doxycycline on restenosis after coronary stenting. In the present study, we investigated whether short-term administration of celecoxib with or without inhibition of MMP using doxycline in the early phase after coronary stent implantation could effectively reduce neointimal hyperplasia.
MATERIALS AND METHODS
Study design and population
The present study was designed as a prospective, open-label, randomized single-center trial with three treatment groups: combination therapy (group I), celecoxib only (group II), and non-therapy control (group III). For 3 weeks after coronary stenting, patients in group I were given celecoxib (200 mg) and doxycycline (20 mg) twice daily; those in group II received celecoxib 200 mg twice daily; and those in group III received neither. A total of 75 patients were enrolled at Severance Cardiovascular Hospital, Yonsei University Health System, from September 2004 to January 2006. Inclusion criteria were as follows: typical angina pectoris or documented myocardial ischemia and significant coronary artery stenosis (>50% luminal narrowing on coronary angiogram) with a reference vessel diameter approximately 2.75-4.25 mm and a lesion length <28 mm. The following exclusion criteria were used: chronic inflammatory disease; autoimmune disease, acute or chronic infection; severe congestive heart failure (New York Heart Association classification >II); left ventricle ejection fraction <30%; hemodynamic instability; clinically significant hemorrhagic episode; warfarin use; hepatic dysfunction (SGOT, SGPT, Bilirubin twice the upper normal limit); active peptic ulcer disease; contraindications to or history of allergy to aspirin, clopidogrel or celecoxib; expected survival of less than 2 years because of medical conditions; pregnancy or desire to become pregnant; chronic total occlusion; saphenous vein graft lesion; or overlapped stenting. Patients already taking any COX-2 inhibitors or any non-steroidal anti-inflammatory drugs were also excluded. All patients provided written informed consent, and the study was approved by the institutional ethics committee. The study protocol was in accordance with the Declaration of Helsinki.
Coronary intervention
All patients received a daily dose of 100 mg aspirin and 75 mg clopidogrel for ≥3 days or a loading dose of 200 mg aspirin and 300 mg clopidogrel before the procedure. A bolus of 100 U/kg heparin was administered after sheath insertion, and supplemental doses were given subsequently to maintain an activated clotting time >300 seconds. Balloon predilation was performed in all patients prior to stent implantation. For coronary stenting, only bare metal stents (Multi-Link Vision®, Guidant, Indianapolis, IN, USA) were used. After stent implantation, patients continued to daily receive aspirin (100 mg) indefinitely and clopidogrel (75 mg) daily for at least 6 weeks.
Follow-up
Patients were clinically followed at 1, 3, and 6 months. Patients were asked specific questions about major cardiac adverse events and the development of angina, according to the Canadian Cardiovascular Society classification of stable angina. Follow-up coronary angiographic and intravascular ultrasound (IVUS) evaluations were performed 6 months after the initial procedure or earlier if symptoms suggestive of coronary restenosis developed before that time.
Quantitative coronary angiography
Angiographic images were obtained in two orthogonal views after intracoronary administration of 200 µg nitroglycerin. Follow-up coronary angiographic images with the same view as those in pre- and post-PCI angiography were used for analyses. Quantitative angiography analysis was performed using an offline system (CMS, Medis Medical Imaging System, Nuenen, the Netherlands) by experienced technicians who were blinded to the patients' clinical data. The minimal luminal diameter (MLD) of treated coronary segments, reference diameter, percent diameter stenosis, and lesion length were measured. The angiographic end points were binary restenosis rate defined as an in-stent stenosis >50% at 6-month follow-up coronary angiography and late loss defined as the MLD after the procedure minus the MLD at 6-month follow-up.
IVUS evaluations
IVUS was evaluated after coronary stenting and at 6-month follow-up using a 2.5 F Atlantis SR Pro Imaging 40 MHz catheter (Boston Scientific, Santa Clara, CA, USA) with an automatic motorized 0.5 mm/s pullback. The coronary segment was examined by IVUS beginning 5 mm distal to and extending 5 mm proximal to the stented segment. All IVUS images were obtained after intracoronary administration of nitroglycerin (200 µg) and recorded on s-VHS tape or compact disk for offline analysis. Quantitative analysis of IVUS was performed using commercially available planimetry software (Echoplaque 2; INDEC Systems, Inc., Mountain View, CA, USA). IVUS measurements were made at 1-mm intervals. Stent and lumen areas were manually traced, and neointimal area was computed as stent minus lumen area. Proximal and distal reference cross-sectional areas were measured at the most visibly normal area (largest lumen with the smallest plaque burden) within 10 mm of the proximal or distal ends of the lesion. Minimal luminal area was defined as the smallest area within the target lesion. Volumes were calculated using Simpson's rule. Vessel volume was defined as external elastic membrane volume. Peristent plaque volume was calculated as vessel minus stent volume. Neointimal volume was calculated as stent minus lumen volume, and neointimal obstruction was calculated as neointimal volume divided by stent volume, expressed as a percentage. Vessel, peristent plaque, stent, lumen, and neointimal volumes were computed for the entire stented segment. To adjust for different stent lengths, the neointimal volume index was calculated as neointimal volume divided by stent length.
Inflammatory biomarkers
Blood samples were collected at baseline prior to PCI and 2 days and 3 weeks after PCI. High-sensitivity C-reactive protein (hsCRP) and MMP-9 in serum were measured using a standardized enzyme-linked immunosorbent assay (ELISA; R&D systems). Serum was separated from whole blood by centrifugation (1,000×g for 15 min) and stored at -70℃ prior to assay. The concentration of soluble CD40 ligand in plasma, obtained from EDTA-treated blood samples as described for serum, was quantified by ELISA (BioSource).
Study endpoints
The primary study endpoint was neointimal volume obstruction on IVUS at 6 months. The secondary endpoints were changes in blood levels of inflammatory biomarkers and angiographic late loss, binary restenosis rate, and major adverse cardiac events, including cardiac deaths, non-fatal myocardial infarctions, and target vessel revascularization.
Statistical analysis
The sample size was calculated based on a two-sample and two-sided test. Previous studies showed that bare metal stents have a neointimal volume obstruction of approximately 30% with a standard deviation of 10% at 6 to 9 months.14-16 We hypothesized that effective inhibition of neointimal hypersia by administration of COX-2 inhibitor with or without MMP inhibitor could achieve a neointimal volume obstruction of about 20%. Based on an alpha level of 0.05, statistical power of 80%, and a drop-out rate of 30%, at least 23 patients were required for each group.
All analyses were performed using the SAS statistical package version 9.1.3. Categorical variables were expressed as percent and were compared using chi-square tests; when the expected cell number was <5, Fisher exact tests were used. Continuous data were expressed as mean±SD and were compared using ANOVAs. For all tests, a two-tailed p-value <0.05 was considered significant.
RESULTS
Patient population
Between September 2004 and January 2006, 75 patients with 86 lesions were randomized into three groups: group I (combination therapy) contained 25 patients with 26 lesions; group II (celcoxib only) contained 25 patients with 28 lesions; and group II (control) contained 25 patients with 32 lesions. The clinical and angiographic characteristics of the patients assigned to the three treatment groups were not different at baseline (Table 1 and 2).
Angiographic data
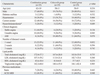
Follow-up angiography at 6 months was performed in 65 patients with 73 lesions. Table 3 shows qualitative comparative analysis outcomes at pre-intervention, just after coronary stenting, and at 6 months follow-up. Late luminal loss and binary restenosis were similar among the three groups. The binary restenosis rate was 28% in the combination group, whereas 25% and 17.9% in the celecoxib-only and control groups, respectively (p=0.666).
IVUS data
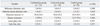
Follow-up IVUS data at 6 months were available for 58 patients with 65 lesions. The interval between baseline and follow-up studies averaged 6.6±1.4 months. Follow-up IVUS data were not obtained in 7 patients with 8 lesions who were followed with coronary angiography due to following reasons: IVUS could not be performed in three patients due to technical constraints such abnormal radial artery variations or extremely tortuous subclavian and brachiocephalic artery for the insertion of guiding catheter. In the remaining four cases, images of IVUS were not obtained because of patient's refusal (n=2) or not analyzable due to poor image quality (n=2). None of these patients showed significant restenosis >50%. Table 4 summarizes the result of IVUS volumetric analysis at the target lesions. There were no significant differences in neointimal volume obstruction or neointimal hyperplasia volume index among the three different treatment groups. Administration of celecoxib with or without doxycycline did not result in reduction of neointimal hyperplasia volumes compared with control therapy at 6 months.
Clinical events
Mean clinical follow-up duration was 191±22 days (maximum, 266 days). There were no cardiovascular deaths, non-fatal myocardial infarctions, or stent thromboses during the study period. Ten patients required revascularization at the target lesions during the 6 months after coronary stenting. The target lesion revascularization rate was not different among the three treatment groups.
Inflammation biomarkers
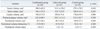
Serum or plasma levels of hsCRP, CD40 ligand, and MMP-9 at baseline prior to PCI, and 48 hours and 3 weeks after PCI are shown in Table 5. There was a general rise in the blood levels of hsCRP, soluble CD40 ligand, and MMP-9 48 hours after coronary stenting. At 3 weeks, blood levels of hsCRP and MMP-9 returned to (or below) baseline values, whereas soluble CD40 ligand levels tended to remain variably elevated. However, there were no differences in biomarker changes at any time point among the different treatment groups.
DISCUSSION
The present study shows that treatment with neither celecoxib alone nor with celecoxib combined with doxycyclin for 3 weeks reduced neointimal hyperplasia at 6 months. Furthermore, neither treatment was capable of reducing blood levels of hsCRP, soluble CD40 ligand or MMP-9 after stent implantation.
A recently published study showed that the adjunctive use of celecoxib for 6 months after implantation of DES reduced the need for revascularization of the target lesion.10 In addition to suppression of inflammatory reactions, inhibition of injury-induced Akt activation has been suggested to be an important mechanism by which celecoxib prevents restenosis after angioplasty.9 Despite the promising results of the study by Koo, et al.,10 however, the beneficial effects of COX-2 inhibition in coronary artery disease have not been consistently supported by other studies. Whereas Wang, et al.8 and Yang, et al.9 demonstrated that selective COX-2 inhibition with celecoxib led to on inhibition of neointimal hyperplasia in different animal models, Connolly, et al.7 reported that COX-2 did not play a role in the development of intimal hyperplasia, despite being expressed in the neointima. Furthermore, the inhibition of COX-2 with rofecoxib failed to improve endothelial function in two clinical trials,17,18 although Chenevard, et al.19 showed that inhibition of COX-2 with celecoxib achieved significant improvement of endothelial function in patients with coronary artery disease. There are also conflicting data with respect to the anti-inflammatory effects of COX-2 inhibition. Although Chenevard, et al.19 and Bogaty, et al.17 reported that inhibition of COX-2 led to reduced levels of inflammatory biomarkers, Koo, et al.10 and Title, et al.18 reported that administration of selective COX-2 inhibitors did not significantly change the levels of inflammatory biomarkers. These conflicting results might reflect the wide variation in baseline inflammatory activity and different extent of vascular injury, as was observed in our study. Furthermore, we cannot rule out the possibility that selective COX-2 inhibitors exert different cardiovascular effects. In fact, Niederberger, et al.20 showed that celecoxib, but not rofecoxib, inhibited the proliferation of vascular cells, and Walter, et al.21 showed that rofecoxib and etoricoxib increased low-density lipoprotein oxidation, whereas celecoxib had no such effect.
In contrast to the study of Koo, et al. we failed to show reduction of neointimal hyperplasia by treatment with celecoxib. There are several differences between these two studies. First, we treated patients with celecoxib for only three weeks after PCI in contrast to the 6-month treatment in the study of Koo, et al. Our intention was to suppress inflammatory reactions only during the early inflammatory phase after vascular injury caused by stent implantation. However, our study results suggest that suppression of early inflammatory reactions after coronary stenting may not be sufficient to reduce restenosis; thus, a more prolonged therapy of celecoxib may be required to suppress neointimal proliferation. As shown in the experimental study by Yang, et al.,9 inhibition of the Akt signaling pathway may be a more dominant mechanism for the reduction of neointimal hyperplasia by celecoxib than suppression of inflammatory reactions. Second, we used bare metal stents in contrast to the paclitaxel-eluting stents used in the study by Koo, et al.10 Accordingly, we cannot rule out a positive interaction between celecoxib and paclitaxel in the reduction of neointimal hyplasia. It is also possible that unsuppressed inflammatory reactions and vascular remodeling after implantation of bare metal stents are more difficult to overcome with celecoxib treatment than the mostly controlled vascular reactions that occur after implantation of drug-eluting stents. However, it would be more desirable to use an additional drug therapy for reducing neointimal hyperplasia in combination with bare metal stents rather than drug-eluting stents, since drug-eluting stents alone have proven to be effective to prevent restenosis. Third, we used IVUS to investigate neointimal hyplasia after stent implantation. IVUS is generally considered a more accurate technique than angiographic assessment.
In the present study, we also investigated the effects of concurrent COX-2 and MMP-9 inhibition using combination therapy with celecoxib and doxycycline, a nonspecific MMP inhibitor. Our hypothesis was that the anti-inflammatory effect of celecoxib combined with prevention of extracellular matrix degradation by doxycycline might synergize to reduce intimal hyperplasia. However, we were unable to demonstrate any beneficial effect of COX-2 and doxycyclin therapy with respect to reducing the levels of inflammatory biomarkers or attenuating neointimal hyperplasia. Because there was no significant decrease in MMP-9 levels in the combination therapy group, we cannot rule out the possibility that the dose of doxycycline was not sufficient to suppress the activity of MMP-9.
There are several limitations in the present study. First, the number of study patients might have been small to detect the difference in neointimal volume obstruction among the patient groups, because the neointimal volume obstruction within the same patient group showed a greater variation than that we have expected. Consequently, the trial might have inadequate statistical power to demonstrate therapeutic effects of celecoxib. Second, there were varied distributions of baseline clinical characteristics among the patient groups because of small study population and non-stratified randomization procedure. Even though the differences were not statistically significant, we cannot rule out that they might have influence on the extent of NIH and restenosis rate. Third, the patients exhibited a wide variation in inflammatory status, which added a level of complexity in evaluating the differences among the study groups. Finally, the time points chosen for evaluation of serial changes in blood levels of inflammatory biomarkers may not have been optimal.
In conclusion, our study failed to demonstrate beneficial effects of the short-term therapy with celecoxib and doxycycline or with celecoxib alone in the suppression of inflammatory biomarkers or in the inhibition of neointimal hyperplasia. Large scale randomized trials are necessary to define the role of anti-inflammatory therapy in the inhibition of neointimal hyperplasia.


 XML Download
XML Download