

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Numerous studies have emphasized the importance of strict blood glucose control for protecting against microvascular and macrovascular diabetic complications.1-4 In addition to patients without overt diabetic nephropathy, the benefits of adequate glycemic control have also been emphasized in patients with end-stage renal disease (ESRD), even after the start of dialysis.2-5 A seven-year observational study with 114 diabetic hemodialysis patients showed significantly higher mortality and worse prognoses in patients with poor glycemic control (HbA1c≥8.0%).6 Shima, et al.7 also reported that intensive management of diabetic control at a stringent mean postprandial glucose level of less than 180 mg/dL could improve the life expectancy of diabetic dialysis patients. Although an issue of considerable debate, currently recommended glucose targets in ESRD patients are identical to those for the general population:8 a fasting blood glucose level below 140 mg/dL, a postprandial value of less than 200 mg/dL, and HbA1c less than 6.5-7%.9-11
To date, HbA1c has been the most widely recognized marker of glycemic control, reflecting one's average glycemic status for the preceding 2 to 3 months.12 However in ESRD patients, the availability of HbA1c is a limitation to its use as a marker of glycemic control, because it can be influenced by various clinical factors such as reduced red-blood cell (RBC) lifespan, recent transfusion, iron deficiency, metabolic acidosis or frequent erythropoietin injection.10-13 As a result, HbA1c tends to underestimate glycemic status, especially in patients with reduced renal function.12,14,15 On the basis of a study involving Japanese hemodialysis patients, serum glycated albumin (GA) has been proposed as an alternative marker of glycemic control in dialysis patients,12 since levels of GA are unaffected by changes in RBC survival time or erythropoietin use.16 Compared to HbA1c, GA responds much sooner to changes in glycemic levels, reflecting short-term glycemic control over the previous 2 to 3 weeks. Furthermore, serum GA may also be a marker of the development of cardiovascular diseases.17 In an observational study by Fukuoka, et al.,5 high GA (≥29%) was a significant predictor of cardiovascular death compared to low GA (<29%), but this was not observed with HbA1c. Similarly, Yamada, et al.18 showed that serum GA level, not HbA1c, is closely associated with peripheral vascular calcification and pulse-wave velocity, an indicator of advanced atherosclerosis and arterial stiffness in diabetic dialysis patients.
Nevertheless, there are some limitations to the use of GA in clinical practice, due to lack of validated reference ranges; even though the GA/HbA1c ratio is usually estimated as 3.0, this empirical estimate has no statistical background.19 Furthermore compared to HbA1c, for which there is an established equation to translate it into average glucose (AG) values,20-22 there have been few reports on the mathematical method of converting GA measurements into easier-to-understand AG levels in ESRD patients, including peritoneal dialysis (PD) patients.
Therefore, we sought to confirm the measurement of GA as a substitute to HbA1c quantification for the accurate assessment of glycemic control in patients with ESRD. Moreover, we attempted to develop an estimating equation for investigating the relationship between GA and AG levels. The optimal target range for GA in diabetic dialysis patients was also examined in this study.
MATERIALS AND METHODS
Study sample
This was a single-center prospective study conducted at Severance Hospital in Korea between March 2010 and October 2010. Type 1 and 2 diabetic ESRD patients as well as non-diabetic patients between the ages of 18 and 70 years were recruited. Diabetic patients received either an oral hypoglycemic agent, insulin or both, and were required to have relatively stable glycemic control as manifested by at least two HbA1c results in the previous six months with no more than 1% difference. Patients were also classified as hemodialysis (HD) or PD group according to modality of maintaining dialysis during the study period. The duration of diabetes was determined based on medical records. For patients not diagnosed at our center, however, the duration was presumed based on the patients' medical history. Non-diabetic patients included those with no history of diabetes, a plasma glucose level <126 mg/dL after an overnight fast, and an HbA1c level <6.5% at the time of presentation. Criteria for exclusion were extremely young or old age, presence of severe diabetic retinopathy, history of recent hospitalization, and non-compliance. Patients with complicated comorbid conditions or who had taken medications that could influence plasma glucose levels during the previous three-month period were also excluded. This study was performed with approval from the local Institutional Review Board, and informed consent was obtained from all participants.
Glucose measurements
To measure casual blood glucose level, all participants were asked to perform four-point daily self-monitoring of capillary blood glucose (SMBG) (OneTouch Ultra; Lifescan, Milipitas, CA, USA) for at least three consecutive days per week for four weeks. Capillary blood glucose was typically tested at fasting (before breakfast), postprandial (120 min after breakfast), postabsorptive (at 5:00 P.M), and at bedtime. To be enrolled in this study, the number of recorded SMBGs must have totaled at least 40 measurements or more during the study period (a minimum of twice a day for at least two days per week).
A small drop of blood obtained by pricking the skin with a lancet was used to measure capillary glucose level, whereas, serum glucose level was determined using a centrifuged blood sample (i.e., serum). While RBCs in whole blood have a higher concentration of protein, serum has higher water content and consequently more dissolved glucose than whole blood. In general, serum glucose level could reach a level equal to capillary blood glucose level multiplied by 1.15. The results of SMBG tests were recorded and any events including overeating, missing a meal, feelings of dizziness, or other symptoms suggesting episodes of hypoglycemia were also documented. To encourage blood sugar testing and to reduce hypoglycemic events, all patients were provided appropriate feedback by dialysis staff once per week. After eight weeks of initial SMBG, all patients were asked to measure follow-up SMBG for two weeks to verify stable glycemic state.
Average glucose levels for each testing (fasting, postprandial, postabsorptive, and bedtime) and the mean glucose value of total SMBG tests were calculated by the area-under-the-curve (AUC) of each glucose profile using the trapezoidal rule.23
Assays of GA and HbA1c
Blood samples for serum GA, HbA1c levels and biochemical parameters including serum hemoglobin, albumin, blood urea nitrogen, and creatinine were obtained at baseline and at the end of 4 and 8 weeks. To confirm the accuracy of SMBG results, fasting plasma glucose were measured weekly at the dialysis center before the start of each session of dialysis and compared with the results of SMBG.
Serum HbA1c levels were analyzed using routine high-performance liquid chromatography (HPLC, Bio-Rad Laboratories Inc., Hercules, CA, USA), and GA level was measured by enzymatic methods using the Lucica GA-L kit (Asahi Kasei Pharma Corp., Tokyo, Japan) with an automatic spectrophotometer. GA level was given as a percentage of GA divided by the total amount of serum albumin.
Statistical analyses
Demographic biochemical data were expressed as mean±standard deviation (SD) or as percentages. Chi-square and independent t-tests were used to compare the DM with non-DM group or HD with PD group. Pearson's correlation coefficients were calculated to assess the strengths of the relationships between clinical variables. Simple linear regression was used to determine the association between average glucose level and GA or HbA1c, and to create a mathematical equation. For regression analysis, GA at 4 weeks and HbA1c at 8 weeks were used in consideration of their reflectiveness on glucose levels for their respective periods. Analyses of the significant contributing factors for GA were performed using multiple regression analysis. Statistical Package for the Social Sciences (SPSS) for Windows Ver. 15.0 (SPSS Inc., Chicago, IL, USA) was used and p-values <0.05 were considered statistically significant.
RESULTS
Baseline characteristics
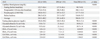
A total of 185 ESRD patients were included in this study. Baseline demographic characteristics of the participants are summarized in Table 1. Two patients had type 1 diabetes mellitus (DM), 152 were type 2 diabetes mellitus and the other 31 were non-diabetic ESRD patients. The median duration of diabetes was 204 (10-600) months. The mean age was 60.3±13.3 years and patients in the DM group were significantly older than those in the non-diabetic group (p<0.001). Patients in the DM group had a higher incidence of cardiovascular comorbidities (p=0.03), but there were no differences in body mass index (BMI), dialysis duration, type of dialysis, and baseline laboratory data between the DM group and the non-diabetic group, except for serum glucose level. In total, 108 (58.3%) patients were on maintenance HD, and 77 patients were undergoing PD. The median durations of HD and PD were 17.0 (9.0-147.0) and 15.0 (9.0-130.0) months, respectively, and the difference was statistically insignificant (p=0.13). When examining the baseline characteristics between HD and PD groups, AG level was similar (166.3±48.6, 172.9±47.7 mg/dL, p=0.350). HD patients were older than those with PD (62.9±12.9 years vs. 56.6±13.1 years, p=0.001) and showed higher serum albumin levels (3.50±0.6 mg/dL vs. 3.21±0.5 mg/dL, p<0.001), compared to PD patients. However, there was no significant relationship between serum albumin and PD duration (r=-0.162, p=0.160) or residual renal function (r=0.086, p=0.785) (data not shown).
Glucose measurements
SMBG by capillary finger stick tests were performed approximately 74.3±7.0 times per each participant (50.5±13.0 times during the initial measurement and 22.5±4.5 times during follow-up). The mean AG calculated by AUC was 169.1±48.2 mg/dL for all subjects, 181.6±42.6 mg/dL for diabetic patients and 106.8±13.9 mg/dL for non-diabetic patients (Table 2). For the follow-up glucose measurement taken at 8 weeks, the calculated AUC was 164.3±44.1 mg/dL, 176.8±37.1 mg/dL, and 100.1±10.9 mg/dL, respectively. Correlation coefficients between the two measurements were r=0.868 (p<0.001), r=0.800 (p<0.001) and r=0.512 (p=0.01), respectively. Based on these data, the glycemic status of the recruited patients was able to be regarded as stable throughout the study period.
As expected, capillary and plasma glucose levels as well as GA or HbA1c were significantly higher in diabetic patients: serum GA and HbA1c were 21.4±6.5% and 7.2±1.1% at 4 weeks and 21.1±6.1% and 7.1±1.3% at 8 weeks, respectively. Whereas, the level of GA and HbA1c in non-diabetic patients was 10.9±2.3% and 6.0±0.9% at 4 weeks and 10.7±1.4% and 5.8±0.4% at 8 weeks. The mean GA/HbA1c ratio (mean values of GA at 4 weeks and HbA1c at 8 weeks) was 3.1±0.8 in the DM group and 1.9±0.4 in the non-DM group; all of these differences were statistically significant.
Moreover, there was a significant discrepancy in GA level dependent upon dialysis modalities. The mean GA level was 20.8±7.3% in HD patients and 17.7±5.9% in PD patients (p<0.001), probably reflecting the lower level of serum albumin in patients undergoing PD. However, no statistically significant difference was observed in HbA1c between these two groups. There were no significant intra-individual variations of GA or HbA1c during the study period.
Correlation between AG and GA or HbA1c
HbA1c and GA levels were proportional to measured AG. The strength of correlation between serum GA and AG levels (r=0.70, p<0.001) was higher than that of HbA1c and AG (r=0.54, p<0.001) (Fig. 1). The correlation had a SD of prediction error of 7.68 mg/dL for GA and 15.83 mg/dL for HbA1c.
Simple linear regression models revealed a close relationship between GA and AG levels and yielded an estimating equation as follows: Mean estimated AG (eAG) (mg/dL)=4.7×GA%+73.35, R2=0.48.
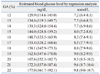
As shown in Fig. 1, the scatter around the regression line was less wide and the slope of the line was significantly steeper between GA and average blood glucose in comparison to those of HbA1c, which supported the hypothesis that HbA1c levels underestimate mean blood glucose levels. Based on the above estimating equation, serum GA values were transformed into their equivalent mean eAG (Table 3). On average, each change of 10 mg/dL in AG level gave rise to 2% changes in GA values. An average blood glucose level of 155-160 mg/dL, which is equivalent to 7% of HbA1c in patients without nephropathy according to the formula of Nathan, et al.,20 was matched to a GA value of 18-19% in patients with ESRD.
Relationships between clinical parameters and GA, HbA1c or GA/HbA1c in diabetic ESRD patients
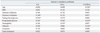
The results of the correlation analyses between various clinical parameters and HbA1c, GA or GA/HbA1c ratio are shown in Table 4. Serum GA level was closely associated with the duration of diabetes (r=0.148, p=0.04) and serum albumin (r=0.260, p=0.01), whereas HbA1c level showed a significant association with only serum hemoglobin (r=0.359, p<0.001). Among the individual time points, some different findings were observed: serum GA level showed higher correlation with postprandial glucose level compared to fasting glucose level (r=0.356, p<0.001 vs. r=0.294, p=0.01). However, serum HbA1c showed the opposite results, which had a higher correlation with fasting glucose level compared to postprandial glucose level (r=0.274, p<0.001 vs. r=0.266, p<0.001). In addition, we also found a strong and significant correlation with bedtime glucose level and GA (r=0.43, p<0.001), suggesting the possible role of bedtime glucose level for determining serum GA level.
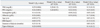
To analyze the independent contribution of clinical factors on serum GA, we constructed a series of multivariate regression models with diabetic ESRD patients (Table 5). In unadjusted analysis (Model 1), fasting and postprandial glucose levels as well as serum albumin levels and dialysis modality were significant predictors in determining serum GA level. Even after adjustment for the clinical and laboratory parameters that might influence serum GA level (Mode 4), a significant positive association of postprandial hyperglycemia (β=0.25, p=0.03) and serum albumin (β=0.17, p=0.04) with GA level was consistently observed, independent of age, BMI, serum hemoglobin, fasting glucose, duration or type of dialysis.
DISCUSSION
Our data convincingly demonstrated that the measurement of GA is a more accurate method of judging glycemic control in ESRD patients. Similar to previous reports, higher explanatory power was observed between AG and GA (r=0.70, p<0.001) compared to HbA1c (r=0.54, p<0.001). Also, we evaluated how to calculate eAG level from GA and developed an estimating equation with a regression line of eAG=4.71×GA%+73.35. Using this mathematical equation, a serum GA level of 18-19% could be matched to an eAG level of 155-160 mg/dL, and each change of 10 mg/dL in blood glucose could give rise to a 2% increase in GA level. Conceptually, converting the GA results into an equivalent "average glucose" level might help our understanding with the interpretation of GA.
To date, serum GA has been suggested as a more reliable and sensitive marker for gestational diabetes, hemolytic anemia and other diseases that shorten the lifespan of erythrocytes,24 while a number of studies have investigated the effectiveness of GA and reviewed its clinical relevance.25 One of them, Inaba, et al.16 confirmed its superiority in 1366 Japanese hemodialysis patients. In that study, HbA1c levels were significantly higher in patients without erythropoietin use, supporting that HbA1c levels are influenced by renal anemia. Peacock, et al.12 also evaluated the accuracy of GA in US diabetic hemodialysis patients and emphasized the importance of GA measurement for long-term glycemic control. However, most previous studies to date have included only hemodialysis patients; therefore, this conclusion might not be applicable to patients with increased albumin loss, as seen in nephrotic syndrome or PD, because albumin leaks into the peritoneal dialysis solution.15 To our knowledge, this is the first study where a generalized estimating equation method was evaluated in all ESRD patients including PD patients.
In our study, the mean GA/HbA1c value was 2.8±0.9 in all participants and 3.1±0.8 in the diabetic group. This result is in good agreement with previous studies and could give additional support to the usually recognized simple equation of GA=HbA1c×3. However, this simple equation might be more suitable for diabetic ESRD patients only, because the GA, HbA1c and GA/HbA1c ratio of non-diabetic ESRD patients was 10.9, 5.8 and 1.9 in our study. Namely, the simple GA/HbA1c ratio of 3.0 could not be applied to non-diabetic ESRD patients. Nevertheless, monitoring of the plasma glucose is also important in non-diabetic patients, since many patients develop diabetes after initiation of dialysis, particularly with PD.26 Therefore, compared to GA, HbA1c and GA/HbA1c ratios, serum blood glucose level could be a more useful tool for screening for the development of diabetes in non-diabetic ESRD patients.
In this study, we also found that serum GA levels were significantly influenced by serum albumin. However, there have been conflicting reports regarding the relationship between serum albumin and GA. Koga, et al.27 reported that serum GA levels could be affected by various conditions with abnormal metabolism of albumin. Under certain conditions with shortened albumin metabolism, such as hyperthyroidism, nephrotic syndrome, PD or administered glucocorticoid treatments, serum GA levels are apparently low, whereas it may be high when albumin metabolism is prolonged, as in liver cirrhosis. However, Inaba, et al.16 could not confirm this finding. In their study with HD patients, serum albumin did not act as a significant determinant of GA. We considered that the conflicting results might come from different ranges of baseline serum albumin concentrations. In our study, serum albumin level widely ranged from 2.3 to 4.9 g/dL and a substantial portion of PD patients showed significant hypoalbuminemia of less than 3.0 g/dL. Particularly, most of these patients revealed lower levels of GA. However, further large-scale studies with heterogeneous dialysis patients are needed to substantiate our observation.
Next, a slight difference in the correlations between GA levels and mean AG values according to each SMBG time point were found. Serum GA levels were more strongly correlated with postprandial glucose level, compared to fasting glucose level. In multiple regression models, only postprandial glucose level was a significant contributing factor for serum GA (p=0.02). Considering that postprandial hyperglycemia is still present in 40% of patients who had achieved their glycemic target and that the loss of postprandial glycemic control is the first step for the deterioration of glucose homeostasis in type 2 diabetes,28 our finding is not surprising and emphasizes the importance of GA monitoring.29 Furthermore, data from large studies underlined the independent role of postprandial hyperglycemia in the increasing risk of mortality.30-32 Even when HbA1c and fasting glucose levels are within normal ranges, postprandial hyperglycemia is associated with a two-fold increase in the risk of cardiovascular mortality.33 Recently, postprandial hyperglycemia has been linked to microvascular complications as well. In Shiraiwa, et al.'s34 study with Japanese type 2 diabetic patients, postprandial hyperglycemia was a strong predictor of the progression of diabetic retinopathy. Therefore, GA values, affected by postprandial glucose level, may be a useful indicator for detecting and preventing diabetic complications.
However, although GA provides a quantitative measure of recent glycemic monitoring, there are some limitations in using only GA as a measure of glycemic control, because this assay does not assess the degree of glycemic variability that a patient may experience within or between days.30 Therefore, SMBG or continuous glucose monitoring (CGM), which reflects daily fluctuations in blood glucose, is necessary.35 In this study, we used SMBG to assess day-to-day variations in average blood glucose levels.
SMBG is frequently used as an adjunctive method for accurate prediction of glycemia, because it provides a real-time measure of blood glucose levels and can detect hypoglycemia or hyperglycemia in detail.30,36 Moreover, it provides immediate feedback to patients and clinicians on therapeutic lifestyles or anti-diabetic medications, which is essential for proper diabetes management.37 Although the optimal frequency and timing of SMBG has not been determined, four to seven times per day is regarded as adequate,30,36 and we used a four-point SMBG method in this study. Considering that every patient in our study was clinically stable during the prescreening and study period, we believe that four measurements of SMBG per day were sufficient.
There are several limitations to the present study. First, we did not perform the continuous glucose monitoring system (CGMS) for measurement of individual glucose levels. CGMS has been recently introduced as a new real-time glucose measurement device. CGMS tests interstitial blood glucose levels every five minutes, and data are transferred to a computer. However, although a CGMS profile provides a more frequent measure of glycemic status, its clinical availability is limited due to high cost. In addition, the results of meta-analysis demonstrated that use of CGMS did not result in a significant reduction in HbA1c (p=0.055) or sensitivity analysis (p=0.775).37 Therefore, SMBG should be regarded as an efficient method based upon its generalizability and cost-effectiveness. Second, there was no analysis of RBC turnover or the dose of erythropoietin use in each patient. Lastly, this was a single center study and a relatively small number of patients were analyzed. Further large-scale observational studies are needed to document the conversion equation of serum GA to mean AG.
In conclusion, our study confirmed the strong relationship between GA and AG levels and provided a direct method to translate serum GA level into an easier-to-understand AG level. Using the estimating equation, an average blood glucose level of 155-160 mg/dL could be matched to a GA value of 18-19% in patients with ESRD.


 XML Download
XML Download