

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Venous thromboembolism (VTE) is a serious clinical condition that manifests as deep venous thrombosis (DVT), pulmonary embolism (PE), or both. PE has a high fatality rate of approximately 15%, exceeding the mortality rate of acute myocardial infarction.1 The likelihood of PE is substantially increased by well-known acquired risk factors and can be significantly reduced by prophylaxis.2 About half of PE cases, however, are idiopathic and occur without acquired risk factors such as antecedent trauma, surgery, immobilization, or diagnosis of cancer.3 Unlike provoked PE (pPE) with acquired risk factors, idiopathic PE (iPE) is less likely to be predicted or prevented.
Hereditary thrombophilia (HT) is considered a major risk factor for idiopathic VTE and its recurrence.4,5 Since the first report of a mutation in the SERPINC1 gene in a family with antithrombin (AT) deficiency, other resulting genetic defects have been identified including factor V Leiden, prothrombin G20210A mutation, protein C (PC) deficiency, protein S (PS) deficiency, and plasminogen (PLG) deficiency. The prevalence of HT varies among different ethnic groups. Factor V Leiden and G20210A mutations are almost exclusively observed in Caucasian populations, while deficiencies of natural anticoagulants have greater implications in Asian populations.6-11 The relative risks for VTE in its various forms of HT are also different.12 A recent study showed that the relative risk for recurrence of VTE was significantly higher in patients with PC, PS, or AT deficiency than in patients with factor V Leiden or G20210A mutation.5 However, there is limited data on the prevalence and clinical implications of HT in VTE in Korea and in other parts of Asia.
This study was conducted to assess the prevalence of HT and its clinical implications in Korean patients with iPE.
MATERIALS AND METHODS
Patient population
We retrospectively collected data from patients diagnosed with PE at Samsung Medical Center between October 2004 and January 2009. The diagnosis of PE was based on multidetector computed tomography (CT) scans including indirect CT venography of the lower extremities. Exclusion criteria were an ethnic origin other than Korean and PE associated with malignancy. We divided the study patients into iPE and pPE groups. The pPE group comprised patients with PE and one or more acquired risk factor of PE (Table 1). All other patients were considered as having iPE. Concurrent DVT in the lower extremities was assessed by CT scan and indirect CT venography, with or without ultrasonography. HT was diagnosed based on coagulation tests. The clinical characteristics and adverse outcomes of iPE with HT (iPE/HT+) group were compared with those of iPE without HT (iPE/HT-) and pPE groups. Adverse clinical outcomes were defined as death; cardiopulmonary resuscitation; thrombolysis; surgical embolectomy; and use of percutaneous cardiopulmonary support, inotropes, or mechanical ventilation. The institutional review board of our institution approved this study.
Coagulation tests for thrombophilia
Coagulation tests to screen for thrombophilia at our center comprise global coagulation tests including prothrombin time, activated partial thromboplastin time (APTT), thrombin time, fibrinogen, PC activity (Stachrom® Protein C, Diagnostica Stago, Asnières, France), PS free antigen (Liatest® Free Protein S, Diagnostica Stago), AT activity (Stachrom® AT III, Diagnostica Stago), PLG activity (Stachrom® Plasminogen, Diagnostica Stago). Lupus anticoagulants (LA) were screened using APTT, LA sensitive PTT (PTT-LA), and dilute Russel veiper venom test on the STA®-Evolution Coagulation Analyzer. Reference ranges for the normal level of each anticoagulant were determined according to our institutional data.
Molecular genetic tests
The diagnosis of HT was also confirmed by molecular genetic tests in available patients with low PC, PS, AT, and PLG on coagulation tests. Genomic DNA was isolated from peripheral blood leukocytes using the Wizard Genomic DNA Purification Kit (Promega, Madison, WI, USA). All exons of the PROC, PROS1, SERPINC1, and PLG genes and their flanking intron regions were amplified using polymerase chain reaction for PC, PS, AT and PLG deficiencies, respectively. Cyclic sequencing was performed using the BigDye Terminator Cycle Sequencing Ready Reaction Kit (Applied Biosystems, Foster City, CA, USA). When no point mutation was identified on direct sequencing, copy number variations were additionally tested by employing the multiplex ligation-dependent probe amplification (MLPA) method, as previously described.14
Statistical analyses
Comparisons of categorical variables were conducted using Chi-square and Fisher's exact tests, where appropriate. Differences in continuous variables were evaluated using univariate analysis of variance. p values less than 0.05 were considered statistically significant. All analyses were performed using SPSS software version 13.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Study patients
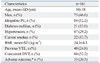
A total of 161 consecutive and unrelated Korean patients with PE were included for analysis. Characteristics of the study patients are summarized in Table 2. Seventy-five patients (46.6%) were male and 86 patients (53.4%) were female. Their age at the time of diagnosis of PE ranged from 13 to 88 years (mean age, 58 years). Eighty-four patients (52.2%) had iPE (52 men and 32 women; mean age, 54 years; age range, 13 to 87 years), and 77 patients (47.8%) had pPE (23 men and 54 women; mean age, 61; age range, 13 to 88 years).
Prevalence of HT and clinical characteristics of iPE with HT
Coagulation tests for thrombophilia were performed in 54 of 84 patients with iPE (64.3%) (Fig. 1). Twenty eight patients (51.9%; 28/54) were diagnosed as having HT (PC, PS, AT, or PLG deficiency), and 26 patients (48.1%; 26/54) were shown to have no evidence of HT.
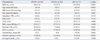
We compared the clinical characteristics among patients in the iPE/HT+, iPE/HT-, and pPE groups (Table 3). The proportion of males to females was highest in the iPE/HT+ group (71.4%) and lowest in the pPE group (29.9%) (p<0.001). The mean age at the time of diagnosis of PE was significantly different among three groups, with the ages of 44±14 years in the iPE/HT+ group, 54±17 years in the iPE/HT- group, and 61±18 years in the pPE group (p<0.001). At the time of PE diagnosis there were no significant differences in the mean systolic blood pressure, mean heart rate, or the frequency of desaturation, defined by oxygen saturation less than 90%. There were no significant differences in the proportion of patients with comorbid diabetes or in regards to the mean body mass index. Hypertension was observed most frequently in patients with pPE. The presence of previous history of VTE was observed most frequently in the iPE/HT+ group (64.3%), followed by those of the iPE/HT- (28%) and the pPE group (10.4%) (p<0.001). The frequencies of concurrent DVT were also significantly different among the groups, with 75.0% in the iPE/HT+ group, 65.4% in the iPE/HT- group, and 46.8% in the pPE group (p=0.021). Hospital stay was longest in the pPE group (27±30, p=0.001). Although there were no significant differences in regards to in-hospital deaths among the groups, adverse clinical outcomes were observed most frequently in the iPE/HT+ group (42.9%), followed by the iPE/HT- group (38.5%) and the pPE group (20.4%) (p<0.001).
Coagulation defects and causative mutations of HT
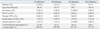
The coagulation defects and clinical characteristics in the 28 patients in the iPE/HT+ group are shown in Table 4. Sixteen patients had PC deficiency, six had PS deficiency, three had AT deficiency, and three had PLG deficiency (29.6%, 11.1%, 5.5%, and 5.5% in 54 patients with iPE, respectively). Although statistical significance could not be assessed due to the limited number of patients with each coagulation defect, those with AT deficiency had the youngest mean age at diagnosis (39±2 years) and the highest frequency of adverse outcomes (100%). Of note, personal history and family history of VTE were similar among the four groups.
Molecular genetic tests were performed in 14 of 28 patients with HT, and the causative mutation was identified in 13 patients (Table 5). Seven patients had a mutation in the PROC gene, three had a mutation in the PROS1 gene, two had a mutation in the SERPINC1 gene, and one had a mutation in the PLG gene. The mean age of the 13 patients with genetically confirmed HT was 43±12 years, and the majority (83%) of them was men. Eight patients (66%) had a previous history of VTE, with a mean age of 39±16 years at first onset of VTE.
DISCUSSION
In this study, we found a high prevalence of HT in Korean patients with idiopathic PE. Up to 52% of patients with iPE had PC, PS, AT, or PLG deficiency. Other recent studies in Asian countries reported that the prevalence of HT in all-cause DVT were 28.3% and 32.1% in Japan and Taiwan, respectively.15,16 Although the prevalence of HT in idiopathic VTE was not known well, a study reported that 67% of patients with idiopathic DVT had one positive marker for thrombophilia including factor V Leiden and prothrombin mutations as well as PC, PS, and AT deficiencies.17 Another study performed in young patients (aged <40 years) with recurrent DVT showed similar results with our study, presenting that a decrease of at least one of PC, PS, and AT levels was observed in almost 50% (15/34) of patients.18
We compared the clinical features of the iPE/HT+ group with those of the iPE/HT- and pPE groups. The iPE/HT+ group had significantly different features, including the youngest age at the time of diagnosis, the highest proportion of male patients, and the highest frequencies of previous history of VTE and concurrent DVT. Interestingly, the age at diagnosis of PE in the iPE/HT- group was between those of the iPE/HT+ and pPE groups (44 years in iPE/HT+, 54 years in iPE/HT-, and 61 years in pPE). These findings suggest that patients with iPE/HT- might have occult predisposition to PE, potentially caused by different genetic backgrounds with a lower risk for thrombosis than natural anticoagulant deficiencies. A Japanese study on patients with DVT showed a similar difference in the ages between carriers and non-carriers of mutations causing natural anticoagulant deficiencies as 44.7 years and 52.6 years, respectively.8 The male predominance in the iPE/HT+ group (71%) was also a notable finding, considering the autosomal dominant inheritance of natural anticoagulant deficiencies and the similar incidences of initial VTE among men and women.19 The gender difference in the prevalence of VTE combined with HT is not well known. The risk of recurrent VTE in men and women, however, was investigated in several studies, and similar conclusions that the risk was higher in men than in women were drawn.20-22 Baglin, et al.20 reported that the recurrence risk was higher in men than in women when only patients with idiopathic VTE were analyzed. Our study showed a higher frequency of female patients in the pPE group. This finding was considered to be due to the fact that orthopedic surgery, connective tissue disease, and pregnancy-related conditions were major risk factors of PE in this study. Our data also showed a higher frequency of concurrent DVT in iPE than in pPE, which is in line with a recent study that showed iPE was more frequent than pPE in PE with DVT than in PE without DVT.23 In addition, the same study showed that natural anticoagulant deficiency was observed more commonly in PE with DVT than in PE without DVT. Lastly, the highest frequency of adverse outcomes was observed in the iPE/HT+ group in this study, suggesting poor prognostic implications of PE in the setting of HT.
It is known that the relative risks for the development and recurrence of thrombosis differ among the different genetic defects implicated in HT.12,24 A recent study in the Netherlands showed that the absolute thrombotic risks in patients with PC, PS, or AT deficiency were much higher than those in patients with factor V Leiden or prothrombin 20210A.12 This finding, along with the prevalence of anticoagulant deficiencies seen in the present study and in other studies from Asian countries,15,16 indicates that tests for HT and risk stratification according to the presence of HT are important in Asian patients with VTE. A study in Taiwan demonstrated that thrombotic risks for PC or PS deficiency are higher than those for AT deficiency or PLG deficiency.9 When we compared the clinical characteristics among four coagulation defects underlying HT, there were differences in the mean age at diagnosis and the frequency of adverse outcomes. Due to the small number of patients, however, the significance of these findings remains indeterminate.
Since coagulation test results are susceptible to underlying disease and anticoagulation, molecular genetic studies provided definitive evidence of HT. Considering this limitation a recent study in Japan investigated the prevalence of natural anticoagulant deficiency in patients with DVT using only genetic tests.8 Their results showed that 55 (32%) of 173 patients carried a genetic defect in one of the PROC, PROS1, or SERPINC1 genes. In our study, the coagulation defect was confirmed using molecular genetic tests in 13 patients in the iPE/HT+ group. Most patients with PROC mutations (85.7%; 6/7) had a missense mutation, either with Arg211Trp or Met406Ile. Both of the mutations were previously reported in Korean male patients with VTE, and Met406Ile was described as a novel mutation.25 Given the findings from the present study, we speculate that Arg211Trp and Met406Ile are frequent mutations causing PC deficiency in Koreans. The remaining mutation of the PROC gene was a novel frame shift mutation (Ala240GlyfsX18 in PC_6 of Table 5). Among the three patients with PS deficiency, one patient (33.3%) had a large copy number variation detected via MLPA analyses (PS_2 of Table 5). This result is in line with a recent series of reports indicating that large copy number variations are uncommonly observed in PS deficiency.13,26,27 The other two mutations of the PROS1 gene were a novel nonsense mutation (Gln572X) and a known missense mutation (Tyr636Cys). One of the two mutations in SERPINC1, Trp81X in AT-1, was a novel mutation, and the Ala620Thr mutation in PLG has been previously reported in Korean patients with DVT.28
This study had several limitations. First, thrombotic profiles tests were not performed in most patients in the provoked PE group. Patients in the provoked group were not tested because most patients in this group had evident risk factors and were relatively old. Therefore, they were unlikely to have HT. Second, as mentioned, about one third of the patients with idiopathic PE were not tested for the presence of HT. Finally, as our analysis was performed retrospectively, there is a chance that personal history or family history for VTE was more enthusiastically detailed in the idiopathic PE group, especially in patients with HT, than provoked PE group.
In conclusion, the present study investigated the prevalence of HT in Korean patients with iPE and revealed that about half of the study patients had a natural anticoagulant deficiency or PLG deficiency. Patients with iPE and HT were mostly young male patients with concurrent DVT, a history of VTE, and a higher frequency of adverse clinical outcomes. Protein C deficiency was the most common genetic defect with recurrent missense mutations. Therefore, it is reasonable to conclude that Korean patients with iPE should be tested for having HT. To investigate the precise prevalence and clinical characteristics of HT in Korean patients with iPE, large-scale prospective study is needed.



 XML Download
XML Download