

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Most patients with newly diagnosed acute myeloid leukemia (AML) will achieve a first complete remission (CR1) with standard induction chemotherapy and require either further (post-remission) chemotherapy or allogeneic hematopoietic stem cell transplantation (alloHCT) for obtaining a durable remission. The decision of which of these options to choose is complex and depends on both clinical and molecular variables as well as the availability and histocompatability of donor stem cells.1
Although karyotype analysis provides a powerful independent prognostic factor for rates of CR, relapse rate and overall survival (OS) in multivariable analyses,2 there are several limitations in the use of karyotype as a risk stratification tool; these include failed cytogenetic analyses, presence of cryptic chromosomal rearrangements and the fact that a substantial proportion of AML cases (-40%) have a normal karyotype.3
Myeloperoxidase (MPO) is the hallmark enzyme of the myeloid lineage. MPO can be detected by cytochemical staining, immunohistochemistry, or flow cytometry. The diagnosis of AML is easy if more than 3% of blast cells are confirmed to be cytochemically MPO positive.4 A few studies have previously shown the prognostic significance of MPO in AML.5-8 However, so far there is no clear explanation on whether the expression of MPO relates to the prognosis of AML.
We retrospectively analyzed the prognostic significance of the MPO expression in the 140 patients with diagnosed AML treated at a single institution.
MATERIALS AND METHODS
Patients
Between January 2006 to August 2010, a retrospective analysis was on 140 patients with newly diagnosed AML (age 15 years or older) treated at the division of hematology, the Yonsei university college of medicine. The diagnosis and classification of AML was determined according to the FAB classification.9 Patient with clinical de novo AML and secondary AML were eligible for this trial; however, patients with FAB AML types M0, M7 [always MPO-negative (MPO-)], or M3 [always 100% MPO-positive (MPO+)] were excluded.
The induction regimen for remission was comprised of idarubicin (12 mg/m2/day I.V. over 30 min on days 1-3) in combination with cytosine arabinoside (ara-C) (100 mg/m2/day I.V. continuous infusion on days 1-7). After achievement of a CR, the options for post-remission treatment were broad and choice of therapy was determined by the prognostic factors at diagnosis and beyond, patient and physician biases. Fifty-five (39%) patients were treated with 2-4 course of post-remission chemotherapy that included high-dose ara-C (3 g/m2 I.V. every 12 hr on day 1, 3, and 5) as consolidation. Thirty-seven (26%) patients who had an available donor, went through alloHCT after several course of post-remission chemotherapy. Nine (16%) were assigned to autologous HCT (autoHCT).
Immunophenotypic analysis
Flow cytometric analysis of bone marrow and/or the peripheral blood cells was performed with an extensive panel of monoclonal antibodies according to (national) protocols currently in use in the different center. The reactivity with anti MPO, CD11c, CD13, CD14, CD15, CD33, CD65s and CD117, referred to as myeloid markers was analyzed. A case was considered to be positive for a marker if ≥20% of the blasts were positive according to EGIL guideline.10 In this analysis, we scored leukemias positive for anti-MPO if >50% of the blasts showed expression.
Cytogenetic and molecular genetic analysis
Chromosome analysis was performed on metaphases from preparations of bone marrow samples. The cytogenetic preparation and G-banding were carried out according to routine laboratory procedure.11 Chromosome was interpreted based on the International System for Human Cytogenetic Non-menclature. Patients were classified into a favorable, intermediate, or adverse risk group based on their karyotypes according to the MRC AML 10 study published.2 Diagnostic samples were also analyzed for mutations in the fms-related tyrosine kinase 3 gene (FLT3) [i.e., the internal tandom duplications (ITDs) and tyrosine kinase domain mutations at codons D835 and I836].
Statistical analysis
Patient characteristics in cases with or without MPO expression by risk factors were compared using the χ2 test in case of discrete variables or using the t-test in case of continuous variables. OS was measures from diagnosis until death from any cause. Patients still alive at the date of last contact were censored at the last follow-up date. Disease-free survival (DFS) was measured from achieving CR until relapse, death from any cause or last follow-up. If patients who were not in remission at the time of transplantation, DFS were measured from the time of transplantation. OS and DFS were estimated using the Kaplan-Meier method, and were compared by the log-rank test according to the MPO expression. Furthermore, the simultaneous effect of risk factors on OS and DFS were analyzed using Cox's proportional-hazard model. Statistical significance is represented by two-tailed p values.
RESULTS
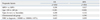
The 140 patients included 81 males and 59 females, with a median age of 51. Table 1 shows the patient's characteristics. Patients were categorized into two groups according to MPO expression; 86 patients (62%) with MPO+ and 54 patients (38%) with MPO-. There were no statistically significant differences in age, sex, presenting white blood count (WBC)type of AML (de novo/secondary), central nervous system involvement at presentation between the MPO+ and the MPO- groups. M1, M2, M4 and M6 were major FAB subtypes in all the MPO groups.
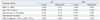
Of the 140 patients who diagnosed AML, 46 (32%) had received transplants, including 37 patients who got alloHCT from a matched sibling (n=21), unrelated (n=16) donor and and 9 patients who got autoHCT (p=0.797) (Table 2). The remaining 94 patients included 55 who received induction and/or post-remission chemotherapy, 39 who received only palliative therapy because of poor performance status or advanced age. Table 3 shows the nature of treatment.
Cytogenetic risk group
In approximately 60% of patients with AML, pre-treatment cytogenetic analysis reveals an abnormal karyotype. Intermediate cytogenetics were relatively common occurring in 62% of cases, and 28 patients were classified in the adverse risk group. MPO expression was associated with favorable cytogenetic risk group (p=0.015). Cytogenetically normal AML was identified in 80 patients (57%), FLT3-ITD was founded in 3 patients (7%) with MPO+ and 3 patients (11%) with MPO- group (p=0.676).
OS and DFS
In this analysis, the median follow-up for the both groups was 12.2 months (range, 0.1-54.1). By the univariate analysis, the age was significant factors associated with OS and DFS (Table 4). The OS at 1 year were 48% in younger age (<60 years) while elderly (≥60 years) was dead within 1 year after diagnosis (p<0.001). The OS was not related with MPO expression (p=0.208) (Fig. 1A). The DFS at 1 year between two age group (<60 vs. ≥60 years) were 34% and 3%, respectively (p=0.019). Patients with MPO- group had an inferior DFS than in MPO+ group (1-year DFS; 26% vs. 50%, p=0.027) (Fig. 1B). In the multivariate analysis, all factors were not significant for OS, but the MPO was associated with better DFS (Table 5). Patients of MPO+ groups had a better DFS than MPO- groups [p=0.049; HR, 0.076; 95% confidence interval (CI), 0.06 to 0.997]. Fig. 2A presents OS and DFS in patients received transplant according to MPO expression. Within 46 patients performed transplant, the median DFS in 28 patients with MPO+ was not significantly different from in 18 MPO- patients (17.5 months vs. 6.8 months; p=0.289). The median OS in the MPO- group was relatively less than in the MPO+ group, but not statistically significant (28.6 months vs. 18.2 months; p=0.375). Also, in patients received an alloHCT (except autoHCT), DFS and OS in the MPO+ group were not statistically different from those in the MPO- group (Fig. 2B).
DISCUSSION
In this study, the DFS of the patients received transplants in the MPO+ group was equal with that in the MPO- group, although the DFS of the all patient in MPO+ group was superior than that in MPO- group. Several studies in AML have examined the prognostic significance of the proportion of MPO+ blast cells. An ECOG study investigated the relationship between MPO+ percentage of blast cells and therapeutic outcomes of 72 patients with AML (FAB M1).6 Thirty-eight patients with low MPO (<50%) group showed a significantly lower CR (52.6%) than the 34 patients with high MPO (>50%) group (85.3%, p=0.003). However, another study of 46 patients with FAB M2 AML reported opposite results that a high proportion of MPO+ blasts before treatment may have constituted a significantly unfavorable prognostic factor.8 So far, the clinical prognostic value of MPO expression in AML has been controversial. In this study, we analyzed the prognostic significance of the MPO expression in 140 patients with diagnosed AML.
The MPO expression was significantly associated with DFS in the overall group, similar to other studies.4-6 Previous report demonstrated that the groups by the MPO expression in the intermediate cytogenetic risk group showed a significant difference in DFS. The DFS rates at 4 years were also different (p<0.001).4
Although our study included a limited number of cases, transplant demonstrated an important role in improving clinical outcomes in AML. There was a significant difference in DFS between the MPO+ group and MPO- group (p=0.027). However, among the patients received transplants, the DFS in overall was not difference in both groups (p=0.289). This results represented that the DFS in the MPO- group was inferior than MPO+ group, but negative prognostic effect was overcame by receiving transplants if suitable donor exist. Previous reports suggested that high relapse rates in patients with AML have led to enthusiasm for the intensification of treatment by the use of high-dose chemoradiotherapy followed by 'rescue' using allogeneic stem cells.12-14 The most important limiting factor for HCT remains the high treatment-related mortality. The long-term mortality from established grade IV GVHD has not changed significantly over the past three decades. The decision to undergo HCT depend on the prognostic factors at diagnosis.15
In conclusion, despite its retrospective study including heterogenous patients with AML and small number of patients, MPO expression was associated with DFS and transplant was beneficial to overcome a negative prognostic effect of MPO- at diagnosis based upon the result that the DFS in patients received transplants are not significant between the MPO+ group and MPO- group although DFS in all patients was different according to MPO expression.
MPO expression at diagnosis in AML patients could be one of the indicators that help identification of patients who benefit from transplantation.





 XML Download
XML Download