

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cytomegalovirus (CMV) infection and disease are important causes of morbidity and mortality among hematopoietic cell transplantation (HCT) recipients.1-4 Among HCT recipients, CMV causes end organ diseases including pneumonia, gastroenteritis, retinitis, and hepatitis. Since the introduction of prophylactic or preemptive therapy against CMV, the incidence of CMV disease has been successfully reduced. However, CMV disease remains one of the major infectious complications after HCT.5 Many factors are associated with the risk of CMV infection and disease. In allogeneic HCT recipients, the serologic status of the donor and recipient was shown to be the most important risk factor for CMV disease.6 Other risk factors for CMV infection include T-cell depletion, acute and chronic graft-versus-host disease (GVHD), the use of mismatched or unrelated donors, and the use of high dose corticosteroid.7-13
Cord blood transplantation (CBT) has become an increasingly utilized method of HCT.14 Cord blood T cells are immunologically naive; therefore, they do not supply passive immunity to the HCT recipient. Although HCT recipients of all donor sources were affected by CMV antigenemia and disease, an increased risk for viral infections after CBT is a concern.4,15,16 Takami, et al.17 reported CBT itself may be correlated with a high incidence of CMV reactivation. Conversely, Walker, et al.12 reported that cord blood (CB) recipients had similar risks of CMV infection, responses to antiviral therapy, and survival following CMV infection as recipients of either bone marrow (BM) or peripheral blood stem cells. Two other studies reported that stem cell source had no effect on CMV infection and disease.18,19 However, only a few studies have examined these relationship between CMV infection and donor source or graft type in pediatric recipients.19 Our study was performed to study this relationship at a single institution with a large pediatric patient population managed consistently by the same physicians.
This study was performed in order to evaluate the incidence and characteristics of CMV infection and disease in children with acute leukemia according to donor source and graft type.
MATERIALS AND METHODS
Study patients and characteristics
A retrospective chart review was performed in children with acute leukemia who received allogeneic HCT at Samsung Medical Center in Korea from October 1998 to December 2009. We excluded recipients who underwent HCT twice or more or who received two or more stem cell sources. In total, 134 patients were included in the analysis. All patients underwent a myeloablative conditioning regimen. Conditioning regimens were chosen depending on underlying diseases, and these were maintained consistently throughout the study period. We identified Samsung Medical Information System's clinical data which included information on age, sex, primary disease, type of stem cell graft, donor source, CMV serostatus of the donor and recipient, conditioning regimen, GVHD prophylaxis, antiviral prophylaxis, the use of anti-thymocyte globulin (ATG), and the presence of GVHD. All included recipients were sorted into the following three groups according to donor source and graft type: CB, related bone marrow or peripheral blood (PB) stem cell (RD), and unrelated bone marrow or peripheral blood stem cell (UD).
Definitions of CMV infection and disease
CMV infection was defined as isolation of CMV or detection of viral proteins or nucleic acid in any body fluid or tissue specimen.20 CMV antigenemia was defined as greater than or equal to 1 CMV pp65 positive cell per 2×105 leukocytes. CMV disease was diagnosed by signs or symptoms and demonstration of CMV infection (upon culture, histopathologic confirmation, immunohistochemical analysis, or in situ hybridization) in organ biopsy specimens. In addition, CMV pneumonitis was diagnosed by interstitial pneumonitis accompanied by CMV antigenemia, unless other pathogens were confirmed. CMV retinitis was diagnosed by typical lesions confirmed by an ophthalmologist. CMV central nervous system (CNS) disease was defined by the identification of CNS symptoms together with the detection of CMV in cerebrospinal fluid samples upon a culture or polymerase chain reaction (PCR).
Recurrent CMV infection was defined as the development of a new positive CMV test occurring after a 50-day interval free of CMV infection. The duration of CMV antigenemia was defined as the number of days from the first detection to the last detection of CMV antigenemia. The total duration of CMV antigenemia was the sum of the duration of all episodes, when recurrent infections occurred.
Management of CMV
Prior to conditioning, CMV serology of the recipient and donor was assessed. CMV immunoglobulin G (IgG) was checked by enzyme linked fluorescent assay. The test was considered positive when CMV IgG antibody level was greater than or equal to 4 AU/mL. The CMV serostatus of cord blood was considered as being negative.21 A CMV pp65 antigenemia test using immunofluorescence stain was performed one to three times weekly after peripheral white blood cell (WBC) count reached greater than or equal to 1.0×109/L. The results of this test were presented as the number of positive cells per 2×105 leukocytes.
Acyclovir was given as a herpes virus prophylactic drug for 4 weeks from the day before transplantation (5 mg/kg/dose q 8 hrs). For CMV prophylaxis, from the 2001 to 2002 period, ganciclovir was used in certain high risk recipients of unrelated donor grafts, but this ganciclovir-based prophylaxis for CMV infection was not used thereafter. Strategies for pre-emptive therapy were maintained throughout the study period, using antigenemia as a surrogate marker for CMV viremia. If CMV antigenemia was detected without evidence of CMV disease, preemptive first-line therapy was started with an induction dose of intravenous ganciclovir (5 mg/kg twice daily i.v.). In patients with a stable condition after post transplant day +30, antiviral therapy was started only when CMV antigenemia was detected above 5/2×105 leukocytes or with increasing CMV antigenemia during follow-up. Foscarnet (180 mg/kg/day i.v. in divided doses) was used in patients with severe neutropenia in place of ganciclovir. A second-line treatment with intravenous foscarnet was generally started in recipients with prolonged CMV antigenemia. Cidofovir or CMV hyperimmunoglobulin was also used for patients who appeared to fail previous treatments. Tests for CMV antiviral resistance mutations were not available.
All packed red blood cells and platelets were transfused using leukocyte-depleting filters and radiation. Granulocyte-colony stimulating factor was given to maintain absolute neutrophil count above 1.0×109/L and total WBC count above 2.0×109/L.
GVHD prophylaxis
GVHD prophylaxis consisted mainly of cyclosporine A (CsA) alone or CsA with other immunosuppressants (mycophenolate, steroid, methotrexate). Protocols for GVHD prophylaxis was consistently maintained, except for CB recipients. CB recipients received CsA and methylprednisolone until December 2004 and received CsA+mycophenolate beginning in January 2005. Most RD recipients and UD recipients received CsA only or CsA+methotrexate, respectively, as the GVHD prophylaxis throughout the study period.
Statistics
Patient characteristics, GVHD, and clinical features of CMV infection and disease were compared across donor sources and types of grafts using the Chi-square test and Fisher's exact test with a permutation method for multiple testing of categorical data. Continuous variables were compared using the Kruskal-Wallis test along with a Tukey test using ranks. The cumulative incidences of CMV antigenemia (for 365 days) and disease (for 730 days) were evaluated using a Fine-Gray regression model.24,25 All statistical analyses were performed using SAS software version 9.1.3 (SAS Institute Inc., Cary, NC, USA) and Stata software version 11.0 (StataCorp LP, 4905 Lakeway Drive, College Station, TX, USA).
RESULTS
Characteristics of patients
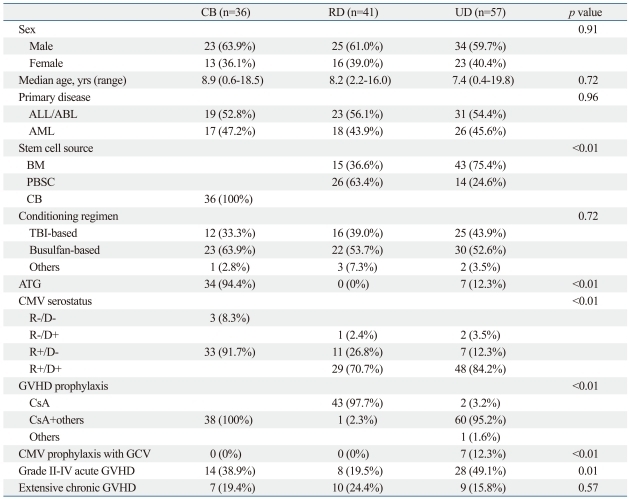
The characteristics of the patients are shown in Table 1. All included recipients were classified into three groups: CB (n=36), RD (n=41), and UD (n=57). These groups were similar with respect to sex, age at HCT, primary disease, and conditioning regimen. The median age of the recipients was 8.2 years. The male to female ratio was 1.6 : 1. ATG was used most frequently in CB (34/36) than the other two groups (p<0.01). The proportion of positive CMV serology recipients was high in all three groups (CB 91.7%, RD 97.5%, UD 96.5%). In addition, the proportion of positive CMV serology donors was high (RD 73.1%, UD 87.7%). All recipients, except for one in the RD group, received only CsA as GVHD prophylaxis, whereas patients in the other groups received CsA plus another immunosuppressant (p<0.01). One of the UD recipients received tacrolimus. Acyclovir was used as herpes virus prophylaxis in all groups. Seven patients in the UD group received ganciclovir in addition to acyclovir. Fewer patients developed grade II to IV acute GVHD in the RD group than other patients (p=0.01). Extensive chronic GVHD occurred similarly among the groups (p=0.53).
Cumulative incidence and clinical features of CMV disease
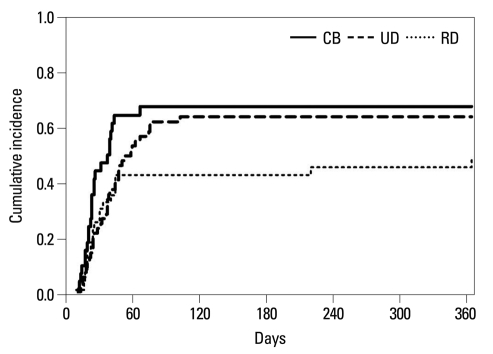
The 365-day cumulative incidence of CMV antigenemia is shown in Fig. 1. The clinical features of CMV antigenemia are shown in Table 2. The cumulative incidence of CMV antigenemia was 67% in CB, 49% in RD, and 65% in the UD group. There was no significant differences among these groups in cumulative incidence of CMV antigenemia. First, CMV antigenemia was detected earlier in CB recipients (p=0.05). CB recipients also had the highest median value of peak CMV antigenemia (CB 160/2×105 leukocytes vs. RD 7/2×105 leukocytes vs. UD 19/2×105 leukocytes, p<0.01). In addition, the duration of CMV antigenemia was the longest in the CB group (CB 87 days vs. RD 17 days vs. UD 28 days, p<0.01). However, the recurrence of CMV antigenemia occurred similarly among all three groups (p=0.77).
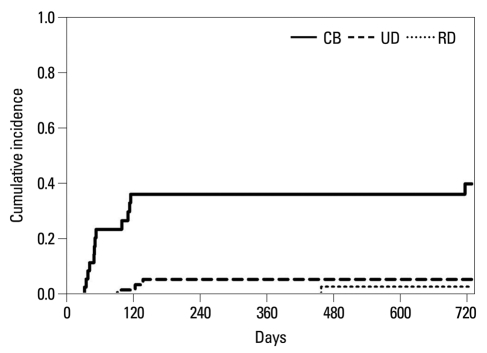
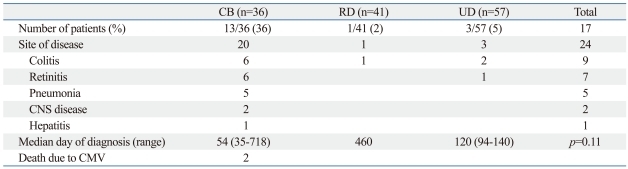
The 730-day cumulative incidence of CMV disease is shown in Fig. 2. The clinical features of CMV disease are shown in Table 3. CB recipients had the highest cumulative incidence of CMV disease (CB 36% vs. RD 2% vs. UD 5%, p<0.01). All of the recipients with CMV disease had CMV antigenemia before the diagnosis of organ involvement. Among all of the groups, 17 patients developed CMV disease at 24 organ sites (colitis in 9 patients, retinitis in 7 patients, pneumonia in 5 patients, CNS disease in 2 patients, and hepatitis in 1 patient). While HCT recipients in the RD and UD groups had only one organ involvement during CMV disease, five of the 13 CB recipients (38.5%) developed multi-organ CMV disease. Three patients had pneumonia plus retinitis. Of which, two patients had three-organ involvements; one patient had retinitis, colitis, and CNS disease; and the other had pneumonia, retinitis, and CNS disease. Among the 17 patients with CMV disease, two patients died of interstitial CMV pneumonitis. Both of them were CB recipients. One was a 12-year old male who received CBT for acute myeloid leukemia. He received multiple immunosuppressive agents to control chronic GVHD. He developed CMV reactivation after the use of alemtuzumab, which eventually progressed to CMV pneumonitis and was not controlled despite aggressive antiviral treatment. The other patient was a 10-month old infant who received CBT for infantile acute lymphocytic leukemia (ALL). He received steroid for GVHD and developed CMV antigenemia at day +28. CMV disease (pneumonitis, retinitis, and CNS disease) was uncontrollable despite treatment. One patient in the RD group developed organ involvement, which was CMV colitis. This patient was a 16 year old male with ALL who received a sibling matched allogeneic bone marrow transplantation. He developed chronic GVHD, which required immunosuppressants including cyclosporine, azathioprine, and mycophenolate. He developed hematochezia for which a colonoscopy was performed and pathologic confirmation was made for CMV colitis. The patient received ganciclovir; however, the general condition was very poor presenting multiple other complications, and he died.
DISCUSSION
Serious CMV infection can complicate the post-transplant course of HCT recipients. Therefore, knowledge on the risk factors of serious CMV infection in HCT recipients is needed in order to care for high risk patients. Little is known about CMV infection in pediatric HCT recipients, according to donor source and stem cell graft type in CMV high-prevalent populations, such as Korea where over 90% of pediatric HCT recipients are CMV-seropositive before HCT. Our current study tried to evaluate the differences in the cumulative incidence and clinical features of CMV infection, according to donor source and graft type in children with acute leukemia. Our study demonstrated that CB recipients had more serious CMV infections and a higher cumulative incidence of CMV disease than recipients of other stem cell sources.
The cumulative incidences of antigenemia were comparable among the three groups (CB, RD, and UD). However, CB recipients had the highest median value of peak antigenemia and the longest duration of CMV antigenemia among all recipients. In addition, the cumulative incidence of CMV disease was higher in the CB recipients than the other groups. Moreover, CMV disease was likely to involve multiple organs in CB recipients. Considering the similar incidences of antigenemia among the three groups, it could be interpreted that a high level of prolonged CMV antigenemia may have caused more CMV disease in CB recipients. Potentially, a high viral load may have contributed to the progression of CMV antigenemia to CMV end organ disease in CB recipients.26
This study revealed that CB recipients had more serious CMV infections and a higher cumulative incidence of CMV disease than recipients of other stem cell sources. There are several reasons that can be considered for the explanation thereof. Firstly, transplanted cord blood stem cells are immunologically naïve.15 Therefore, recipients do not receive passive immunity from CB. Previous studies reported fewer CMV-specific T cells and a higher incidence of viral infections after CBT.19,27-29 Secondly, reconstitution of CMV-specific cytotoxic T lymphocytes response after HCT correlates with protection from CMV and improved outcomes of CMV disease.30-34 Post-transplant immune recovery is delayed in CBT and CB recipients may have more profound impairment against CMV infection.27,28,35 Thirdly, ATG may have affected the high cumulative incidence and serious disease course of CMV infection, since ATG was given to most of the CB recipients. Therefore, the risk of infection, including CMV disease, appears to have increased when high doses of ATG were employed in myeloablative conditioning.36 CMV reactivation is controlled by CMV-specific T cells.37,38 ATG possibly damaged recipient-derived anti-CMV immune cells, which may have been important because CB recipients can not gain anti-CMV immunity from the donor stem cells.
Improvement of diagnostic methods and antiviral agents has enabled early detection of CMV to prevent reactivation and subsequent development of CMV diseases. Recent guidelines recommend antiviral prophylaxis with CMV reactivation screening or empiric treatment.31 When prophylaxis is chosen against CMV infection, chemoprophylaxis is recommended from the engraftment until at least day +100 after HCT. Otherwise, all allogeneic recipients including CB recipients should receive preemptive treatment when any level of CMV PCR or antigenemia was detected during less than 100 days post-HCT. In our institution, acyclovir prophylaxis was given until day +28 for herpes virus infection and preemptive treatment was given later, when CMV antigenemia was detected during follow-up. All of our CB recipients developed CMV infection before day +100 post-HCT.
There are many reports being published in the field of transplant-related CMV infection. Our study is limited in that the data were collected retrospectively from a single center that included only pediatric patients with leukemia. However, we tried to select only patients with leukemia to reduce the heterogeneity among patients.
In conclusion, in pediatric patients with acute leukemia who received allogeneic HCT, CBT was associated with increased risk of prolonged CMV antigenemia, higher viral loads, and more serious CMV diseases compared to unrelated or related PB or BM allogeneic HCT recipients.

 XML Download
XML Download