

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Atopic dermatitis (AD) is a common chronic relapsing inflammatory skin disease characterized by itching, dry skin, inflammation and exudation frequently associated with a personal or familial history of allergic diseases.1 Allergic response to common environmental agents (allergen) has been suggested as one of major pathogenetic mechanisms responsible for the development and maintenance of chronic skin inflammation in patients with AD.2
Current standard medical therapies for AD using topic corticosteroids and/or lotopical calcineurin inhibitors are mainly focused on transient improvement of inflammation and clinical symptoms, and their long-term clinical efficacies are often disappointing to both patients and physicians.3 Although a significant number of patients with severe AD can be improved by the treatment with systemic corticosteroids, cyclosporin, or mycophenolate mofetil, the possibility of systemic toxicities from these medications restricts a long-term clinical application.3
Subcutaneous allergen immunotherapy (SCIT) is a treatment of administering gradually increasing doses of allergen to patients with allergic diseases by subcutaneous injections in order to decrease a hypersensitivity to the allergen and thereby reduce clinical symptoms from exposure to the allergen.4 The clinical efficacy of SCIT has been proven for the treatment of allergic rhinitis, allergic asthma, and Hymenoptera hypersensitivity.4,5 It can alter the natural course of respiratory allergic diseases, prevent the development of new allergen sensitizations, and produce a sustained clinical improvement after discontinuation of the treatment.5
Clinical usefulness of SCIT for AD is still controversial.3 However, an increasing amount of evidence indicates clinical efficacy of SCIT for the treatment of AD.6 SCIT with house dust mite (HDM) extract has been shown to be clinically beneficial in patients with severe AD in a randomized controlled study.7 However, compliance rate of the above randomized study was about 50% at the end of 1 year treatment period.7 The clinical efficacy of SCIT is not satisfactory in some patients with severe AD.7 Recently, we have tried combined treatment with SCIT and a histamine-immunoglobulin complex in patients with recalcitrant AD to improve the clinical efficacy of SCIT.8 However, there are needs for further development of additional therapeutic modalities for patients with severe AD.
We hypothesized that combined treatment with SCIT and cyclosporin could provide further long-term clinical improvements in patients with severe AD by reducing allergic inflammation through induction of allergen-specific immune tolerance together with non-specific immune suppression. Here we report results of an uncontrolled pilot study in which patients with severe AD and hypersensitivity to HDM were treated with a combination of SCIT and cyclosporin.
MATERIALS AND METHODS
Patients
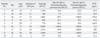
Nine patients (4 females and 5 males) between 13 and 36 years of age (20.7±8.4; mean±SD) with severe recalcitrant AD who fulfilled all of the criteria below were included in the study (Table 1). The patients showed the typical clinical features of AD compatible with the diagnostic criteria for AD, suggested by Hanifin and Rajka.9 In this study, severe recalcitrant AD was defined when clinical conditions of the patients had not been effectively controlled by current standard medical therapies (topical moisturizers, topical corticosteroids, topical calcineurin inhibitors, and oral antihistamines) and clinical severity scoring system for atopic dermatitis (SCORAD) values of the patients were greater than 50 as previously described.8,10 All patients showed strong positive results on serum-specific IgE antibody tests to HDM (≥3.5 kU/L) by CAP-FEIA (Phadia, Uppsala, Sweden), and they all provided written informed consent. This study was performed in accordance with local clinical practice guidelines, and was approved by the institutional review board.
Preparations for treatment
A HDM allergen extract containing a mixture of Dermatophagoides farinae and Dermatophagoides pteronyssinus extracts (50 : 50%), which was adsorbed to aluminum hydroxide (Novo-Helisen Depot®; Allergopharma Joachim Ganzer KG, Reinbeck, Germany) was used. The concentration of HDM allergen extract for maintenance immunotherapy was 5,000 therapeutic units/mL according to the manufacturer. The histamine-immunoglobulin complex (Green Cross PBM, Seoul, Korea) contained 12 mg of human immunoglobulin and 0.15 µg of histamine dichloride.
Allergen immunotherapy
In this study, ultra-rush immunotherapy schedule was applied to shorten the initial build-up phase of SCIT and provide a rapid onset of clinical efficacy as previously reported.11 All patients received premedications which consisted of fexofenadine 120 mg/day and ebastine 10 mg/day during the ultra-rush immunotherapy to minimize systemic allergic reactions. For ultra-rush immunotherapy, patients were admitted to the hospital, and 0.1 mL, 0.2 mL, 0.4 mL and 0.8 mL of maintenance concentrations of HDM allergen extracts were injected subcutaneously to the patients at 2 hour intervals for 6 hours, and they were then observed overnight for possible developments of delayed-onset systemic reactions. Then, 0.8 mL of maintenance concentration of HDM allergen extract was injected subcutaneously once monthly as a maintenance treatment in out-patient clinic. The total duration of SCIT was 12 months in this study.
To improve the clinical efficacy of SCIT for AD, 0.8 mL of maintenance concentration of HDM allergen extract was mixed directly with the histamine-immunoglobulin complex and the mixture was injected subcutaneously into the upper arm at each time scheduled for maintenance treatment as previously reported.8
Standard medical therapies
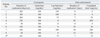
Standard medical therapies including topical moisturizers, topical calcineurin inhibitor, topical corticosteroids, and oral antihistamines were maintained throughout the study period. Short-term treatment with low-dose oral corticosteroids (≤10 mg of prednisolone/day or an equivalent dose of other corticosteroids for fewer than 50 days/year) was allowed for the management of acute exacerbations. The timing, dose, and duration of oral corticosteroid treatment were recorded (Table 2).
Cyclosporin treatment
Oral cyclosporin treatment was started with SCIT in the patients because uncontrolled severe clinical symptoms from AD inhibited normal daily life of patients during the standard medical therapies (Table 2).
The initial dose of cyclosporin was 100 mg/day and the dose of cyclosporin was increased to 200 mg/day to control the clinical symptoms of AD after 4 weeks if patients tolerated the dose of cyclosporin without evidences of gastrointestinal, hepatic or renal toxicities. If the clinical symptoms of AD were controlled in the patients, we tried to reduce the dosage of cyclosporin every 4 weeks according to the therapeutic response, and discontinued if the clinical symptoms could be controlled by standard medical therapies and SCIT. Liver and kidney functions were checked by blood tests at monthly intervals during the cyclosporin treatment. The timing, dose, and duration of cyclosporin treatment were recorded.
Assessment of outcomes
The primary efficacy outcome was the change in the SCORAD values, measured at 6 and 12 months, in comparison with the values at baseline as previously described.10
RESULTS
Compliance and side effects
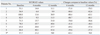
One of the 9 patients enrolled in the study was lost to follow-up at 8 months after the treatment due to noncompliance (Table 3). The patient did not experience significant side effects from the treatments or significant acute exacerbation of AD during the treatment. The other 8 patients completed 12 months of combined treatment with SCIT and cyclosporin. Generalized urticaria was observed in 2 patients among 9 patients during ultra-rush immunotherapy. Urticaria was rapidly resolved following intravenous administration of 4 mg of chloropeniramine and 5 mg of dexamethasone. No other significant systemic side effects were observed in the participants.
Clinical efficacy
In 8 patients who completed all 12 months of treatment, the SCORAD values decreased significantly from 71.5±15.5 (mean±SD) at baseline to 20.4±14.6 at 6 months and 26.3±13.6 at 12 months (Wilcoxon signed-rank test, p=0.01, at 6 months and 12 months compared to the baseline) (Table 3, Fig. 1). Cyclosporin was discontinued in 4 of 8 patients within 8 months after starting the combined treatment (Table 2).
A decrease of SCORAD value ≥50% from baseline value (clinical improvement of AD ≥50% compared to baseline: ADI50) was observed in 6 (75.0%) of 8 patients after 12 months of treatment (Table 3).
Oral corticosteroids (≤10 mg prednisolone/day or an equivalent dose of other corticosteroids) were administered in 6 of the 9 patients due to temporary acute exacerbation of AD during the treatment period. However, the total duration of oral corticosteroid treatment was less than 50 days in each patient (Table 2).
DISCUSSION
In this uncontrolled pilot study, combined treatment with SCIT and cyclosporin significantly improved the clinical severity of patients with severe recalcitrant AD whose clinical conditions had not been effectively controlled by current standard medical therapies. In addition, the combined treatment was well tolerated in this study and produced no significant systemic side effects.
There have been numerous studies on the clinical efficacy of SCIT for the treatment of AD.12 SCIT with HDM extract has been shown to be clinically beneficial in patients with severe AD in a randomized controlled study.7 However, the compliance rate of the above randomized study was about 50% at the end of 1-year treatment period.7 A significant clinical improvement, defined as a decrease of clinical severity score for AD values ≥50% from baseline value (ADI50), was observed in only 3 (33.3%) of 9 patients with severe AD after 12 months of combined treatment with SCIT and a histamine-immunoglobulin complex.8 In the present study, it was of an interest to observe that significant clinical improvement (ADI50) was achieved in 6 (75.0%) of 8 patients with severe AD who received 12 months of combined treatment with SCIT and cyclosporin. Further studies to improve clinical efficacy and compliance of SCIT for the treatment of patients with severe AD are needed.
Allergen immunotherapy has been shown to provide a long-lasting suppression of hypersensitivity to allergen and modify a natural course in patients with respiratory allergic diseases.13,14 Currently available medical therapies for AD are designed to temporarily improve the clinical symptoms during medication.12 Although there have been limited numbers of studies on the clinical efficacy of allergen immunotherapy for AD, allergen immunotherapy could provide long-term stabilization of AD.15 Cyclosporin has been regarded as the most effective medication for short-term treatment of severe AD because of rapid onset of clinical efficacy.16 Cyclosporin is licensed in North America and Germany for the short-term treatment of adults with severe AD in whom conventional therapy is ineffective or inappropriate.16 However, the possibility of systemic toxicities from cyclosporin frequently limits their long-term clinical application.16 We hypothesized that a combination of allergen immunotherapy with cyclosporin treatment in patients with severe AD could provide both rapid onset of clinical improvement by cyclosporin treatment and long-term stabilization of disease activity by allergen immunotherapy. Rapid onset of clinical improvement provided by cyclosporin treatment might also improve a long-term compliance of allergen immunotherapy in patients with severe AD. In this study, the combined treatment with SCIT and cyclosporin resulted in significant clinical improvements in patients with severe AD, and cyclosporin treatment could be discontinued in 4 of 8 patients with severe AD who completed SCIT for 1 year. These results suggest that cycloporin treatment could be a useful adjuvant therapy for SCIT in patients with severe AD, like a successful clinical application of short-term oral corticosteroid therapy combined with slow-acting anti-rheumatic medications for patients with rheumatoid arthritis (so called "bridging therapy with oral corticosteroid") to provide fast and sustained clinical improvement.17 Nevertheless, further studies are needed to evaluate the clinical usefulness of this combined treatment with SCIT and cyclosporin for severe AD.
There are contradictory aspects on the immunological mechanisms of therapeutic efficacy of SCIT and cyclosporin treatment for AD. The main mechanism of SCIT was suggested as allergen-specific T cell tolerance associated with the induction of allergen-specific regulatory T cell.18 The key immunological mechanism of cyclosporin is an inhibition of calcineurin-dependent pathways of T cells and subsequent nonspecific suppression of T cells by modulating cytokine transcription.3 Theoretically, cyclosporin treatment might inhibit immunological changes produced by allergen immunotherapy in patients with AD. In this study, cyclosporin treatment could be discontinued in 4 patients among 8 patients with severe AD who completed 1 year of SCIT. This result suggests that SCIT could provide long-term clinical improvement even in patients with severe AD on cyclosporin treatment. However, the precise immunopharmacological mechanism of this combined treatment should be further investigated.
There are limitations of this study in providing clear evidence for clinical efficacy of the new combined treatment. Our study can not escape from a criticism on the need of randomized placebo-controlled demonstration of the clinical efficacy because significant placebo effects have been observed in the previous studies of SCIT in patients with AD and HDM hypersensitivity.6,7 In this study, we used three types of different therapeutic modalities to improve clinical efficacy for the treatment of severe AD which consisted of accelerated schedule of SCIT (ultra-rush immunotherapy), combined treatment with SCIT and cyclosporin, and combined treatment with SCIT and histamine-immunoglobulin complex. Our study also can be subjected to a criticism whether additional effect or synergistic effect was produced from the above 3 different therapeutic modalities.
The management of severe AD is still a challenging issue for both clinicians and patients.3 Recent clinical trials with monoclonal antibodies (anti-IgE antibody, anti-activated T cell antibody, anti-B cell antibody) for the treatment of severe AD produced conflicting results.19-21 Therefore, there are needs for further development of additional therapeutic modalities for patients with severe AD. However, development of entirely new therapeutic modality for severe AD seems to be very difficult in these days because of various regulatory restrictions, costs for clinical trials, and/or risks of unexpected toxicity during the new drug developments. We suggest that trials to combine pre-existing multiple therapeutic modalities could be one way to improve quality of life in patients with severe AD.
In this uncontrolled pilot study, combined treatment with SCIT and cyclosporin resulted in significant clinical improvements in patients with severe AD. Further controlled studies are needed to evaluate clinical usefulness of this combined treatment for severe AD.

 XML Download
XML Download