

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Epidermoid tumors are rare lesions, accounting for 0.7-1.8% of all intracranial tumors.1,2 They are believed to be non-neoplastic lesions and to arise from ectopic ectodermal cells. Although the vast majority of epidermoid tumors are intradural, extradural locations have also been reported.3 The most common locations are the cerebellopontine angle, parasellar area, and middle cranial fossa.1,4 Cavernous sinus (CS) involvement is rare. To the best of our knowledge, there have been only 18 cases in the literature describing the microsurgical management of epidermoid tumors located in the CS.1-5 We present herein a case in which we used an endoscope to assist microsurgical removal of an epidermoid tumor from the cavernous sinus.
CASE REPORT
A 21-year-old male presented with progressive headache, diplopia, and visual disturbance. He exhibited ptosis of the eyelid as well as limited movement of the right eye. Magnetic resonance (MR) imaging showed a well demarcated mass (28×21×21 mm) that was slightly hypointense on T1-weighted images, hyperintense on T2-weighted images, and hyperintense on diffusion-weighted images. MR spectroscopy showed an increased lactate peak. The patient had undergone gamma knife radiosurgery two years previously at an another institution for the treatment of his lesion without a tissue diagnosis.
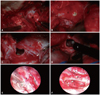
A right frontotemporal craniotomy was performed. An extradural approach to the cavernous sinus was followed after mobilization of the lateral wall of the cavernous sinus. The mass was visualized to protrude laterally through the thickened and fibrotic cavernous sinus wall. The identification of the cranial nerves within the cavernous sinus was challenging despite the use of an intraoperative microscope. Therefore, a very small incision was made between what we believed to be the trochlear nerve and the ophthalmic branch of the trigeminal nerve. A yellowish-white liquid was egressed and suctioned out from the incision (Fig. 1). Then, a neuroendoscope, which measured 18 cm in length and 4 mm in diameter with 30° rod lenses (Karl Storz, Tuttllingen, Germany) was advanced through the small opening. Using the endoscope, a glistening white cauliflower-like mass adherent to the inner layer of the wall of the cavernous sinus was identified. Under a 0° rod endoscopic view, a micro cup pituitary forcep 1 mm in diameter (Codman, Raynham, MA, USA) was inserted together into the cavernous sinus for piecemeal resection of the tumor. It was difficult to manipulate a straight forcep in a single 0° rod endoscopic view. Therefore, at the edge of the inner wall of the cavernous sinus and the carotid artery, 30° and 70° rod lenses were used to provide a variety of angled views. Wide viewing angles allowed us to visualize every corner of the cavity without any blind spots, although we worked through a narrow corridor that permitted only one each of endoscope and a single-shaft micro-forcep. Finally, using a 0° and 30° rod endoscope, gentle irrigation with saline was performed in the hollowed cavity. Following the gross total removal of the tumor including the capsule, the cavernous segment of the internal carotid artery (ICA) as well as parts of the thinned nerve fibers on the wall were visualized (Fig. 1). These nerves could not be visualized in their entirety, likely due to inflammation and fibrosis caused by previous radiosurgery. Even the plane between the nerves and a layer of the cavernous sinus was impossible to identify beyond dissection. A portion of the tumor encased the ICA and abducens nerve. Nevertheless, this tumor portion was meticulously dissected away. Another portion of the tumor extended intradurally above the tentorial hiatus, and was removed with a micro-pituitary forceps without necessitating further incision. The arachnoid was not violated.
The patient's postoperative course was uneventful with immediate improvement of his headache. MR imaging performed on the first postoperative day showed complete removal and signal change, especially in diffusion-weighted MR images (Fig. 2). However, the patient's oculomotor nerve palsy did not improve. Histopathologic examination of the surgical specimen revealed a cystic tumor lined with simple stratified keratinizing squamous epithelium, confirming the diagnosis of epidermoid tumor (Fig. 3). There were no signs of recurrence during a 2-year follow-up.
DISCUSSION
Epidermoid tumors are benign pearly cystic lesions lined with simple stratified keratinizing squamous epithelium.2,6 According to Kaido, et al.,7 during closure of the neural tube, ectodermal cells are sometimes left within the neural tube, and remain entrapped in the meninges around the nerves and grow gradually by spreading in the cisterns enveloping neurovascular structures of the skull base.
Epidermoid tumors are rarely located in the cavernous sinus. Gharabaghi, et al.1 describe three different types of epidermoid tumors of the cavernous sinus. The first is extracavernous in origin and invades or compresses the cavernous sinus. The second originates in the lateral wall of the cavernous sinus and is located interdurally between the inner and outer layers of the lateral wall of the cavernous sinus.3 The third consists of the true intracavernous epidermoid tumors, which tend to encase the ICA, encircling and displacing the cranial nerves laterally. Our case falls into the third group. In general, surgical management of the third type of epidermoid tumors is fraught with challenges, such as limited exposure without retraction of the cranial nerves. Therefore, a variety of surgical strategies have been described. Ikezaki, et al.5 reported a case of a purely intracavernous epidermoid tumor, which was surgically removed via a pterional approach utilizing Dolenc's anterolateral triangle. Because of the difficulty encountered in identifying the abducens nerve, the removal of the capsule in its entirety was not possible so as not to cause abducens nerve palsy. On the other hand, Sekhar, et al.8 described a case of total removal, including the tumor capsule along with the invaded oculomotor nerve, following the reconstruction of sural nerve. However, the patient in this case had already oculomotor nerve palsy.
Fries and Perneczky9 described the advantages of the endoscope as an adjunct tool in microsurgery, including reduced surgical trauma, especially in avascular lesions such as epidermoid tumors. Our goal in using the endoscope was to minimize the risk of neurovascular injury and achieve better exposure. In our case, after intracapsular tumor removal, the remaining parts of the lesion were visualized through the endoscope without any retraction of the cranial nerves. Despite this advantage, the outcome of the patient's cranial nerve functions was not as favorable as that of his pain symptoms. It is possible that the patient's previous radiosurgery might have contributed to this outcome. Although the endoscope offers certain advantages such as better intraoperative visualization, minimization of surgery-related trauma, shorter hospital stays, shorter recovery periods, and less postoperative discomfort, there are certainly some limitations. First of all, the images obtained via an endoscope are two-dimensional. Second, it is challenging to maintain visualization and control in cases of severe bleeding, although epidermoid tumors are not vascular. The third limitation is heat injury to nearby cranial nerves as a result of high temperature generated on the tip of the endoscope by the light source. Therefore, continuous cold irrigation or turning off the light periodically during long operations is advisable.
In summary, epidermoid tumors are benign lesions, however, when located in the cavernous sinus, they pose a number of challenges from the standpoint of surgical management. In this context, endoscopes may assist in achieving adequate exposure, minimizing surgical trauma and improving the extent of resection.


 XML Download
XML Download