

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Highly active antiretroviral therapy (HAART) leads to a spectrum of metabolic complications, including lipodystrophy (LD), insulin resistance (IR) and dyslipidemia,1 that contribute to a higher prevalence of metabolic syndrome (MetSyn) and cardiovascular disease (CVD) in HIV-infected subjects.2-4 Therefore, early detection of MetSyn in these subjects may be important to preventing CVD. Recent studies have reported that retinol-binding protein-4 (RBP-4) is associated with IR,5,6 dyslipidemia7 and obesity,8,9 as well as the components of MetSyn,6,7,9,10 in various non-HIV-infected populations. However, whether serum RBP-4 levels may serve as a risk marker for MetSyn in HIV-infected subjects has not been investigated. The aim of this study was to evaluate the associations between serum RBP-4 levels and MetSyn in HIV-infected subjects receiving HAART.
A cross-sectional study was performed on 98 HIV-infected Koreans at Severance Hospital, Yonsei University Medical Center. We prospectively enrolled HIV-1-infected subjects between March 2007 and March 2008. Patients were eligible if they were between 20 and 80 years old and had been receiving HAART for at least 6 months. We excluded patients who had ever taken anti-obesity medications, corticosteroids, peroxisome proliferator-activated receptor-gamma (PPAR-γ) agonists, statins or fibrates, or had a history of diabetes mellitus or CVD. This study was approved by the Institutional Review Board of the Clinical Research Institute of Severance Hospital. Written informed consent was obtained from all participants.
MetSyn was diagnosed according to the Adult Treatment Panel III criteria when three or more of the following five criteria were fulfilled: blood pressure (BP) >130/85 mm Hg or current use of anti-hypertensive drugs, fasting plasma glucose >110 mg/dL, high-density lipoprotein (HDL)-cholesterol <40 mg/dL in men or <50 mg/dL in women, triglyceride (TG) >150 mg/dL, and abdominal obesity (waist circumference >90 cm in men or >80 cm in women according to the standards of the Asia-Pacific region).11,12 LD diagnosis was based on the clinical definition set by the US Division of AIDS adverse events (2004 version), in addition to a standardized LD-specific physical examination conducted by a single clinician and a previously described LD-specific questionnaire completed by the patient.13 BP, height, weight, and waist and hip circumference were measured. Waist-to-hip ratio (WHR) and body mass index (BMI) were also calculated.
We obtained blood samples following a 12-hour overnight fast. Plasma glucose, total cholesterol, triglyceride, HDL-cholesterol, peripheral blood CD4+ T lymphocyte counts, and plasma HIV-RNA were measured using standard laboratory methods. Low-density lipoprotein-cholesterol was calculated using the Friedewald formula,14 except in patients with TG levels higher than 400 mg/dL.
Serum RBP-4 concentrations were measured using the commercially available human RBP-4 sandwich enzyme-linked immunosorbent assay kit (Immunodiagnostik AG, Bensheim, Germany). The assay was conducted according to the manufacturer's instructions. The inter-assay and intra-assay variations were 9.8% and 5%, respectively.
All statistical analyses were performed using the SPSS 13.0 software (SPSS Inc., Chicago, IL, USA). Data were expressed as means±SD, medians (interquartile range) or numbers (%). The two-tailed unpaired Student's t-test or Mann-Whitney U test was used to compare the mean or median values of continuous variables. To analyze the differences in nominal variables, we performed a chi-square test or Fisher's exact test. To identify clinical parameters associated with RBP-4, a stepwise multivariate linear regression analysis was performed for age, BMI and all variables with a p-value of less than 0.10 on an age and BMI-adjusted partial correlation analysis. p-values <0.05 were considered statistically significant.
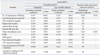
Thirty-three (33.7%) subjects fulfilled the criteria for MetSyn. The numbers of subjects per number of MetSyn components presented, from 0 to 5, were 9, 25, 31, 18, 12 and 3 in respective numerical order. The subjects with MetSyn were older and had significantly higher BMI and WHR than subjects without MetSyn. The percentage of patients with LD was higher in the group with MetSyn (45.5% vs. 23.1%, p=0.041). Also, serum RBP-4 level was significantly higher in subjects with MetSyn (33.87±7.72 vs. 29.85±7.15 µg/mL, p=0.012) (Table 1).
Serum RBP-4 levels were significantly, positively correlated with the number of components of MetSyn presented, TG, waist circumference, WHR and BMI without adjustment. After adjustment for age and BMI, the significant correlation with serum RBP-4 levels was sustained for the number of components of MetSyn presented, TG and waist circumference. The total duration of HAART and known duration of HIV infection had no correlation with serum RBP-4 levels (Table 2). Subjects that presented with 3 or 4 components of MetSyn demonstrated significantly higher serum RBP-4 levels than subjects that presented with none or only 1 component of MetSyn (Fig. 1). In stepwise multivariate linear regression analysis, we identified the number of components of MetSyn and waist circumference as the variables most strongly associated with RBP-4 (Table 2).
Metabolic and body fat abnormalities are common side-effects in HIV-infected subjects receiving HAART, and several reports have suggested that these subjects also involve an increased risk of CVD.15,16 Although the mechanism is not completely understood, adipocytokines such as adiponectin and leptin might contribute to the clinical features of this condition.17 Adipose tissue is considered to be an endocrine organ, and the hormonal alterations caused by changes in body fat may play an important role in metabolic abnormalities in HIV-infected subjects receiving HAART.17 Therefore, we investigated the relationship between serum levels of RBP-4, an adipocytokine, and MetSyn in HIV-infected subjects receiving HAART.
In this study, elevated serum RBP-4 levels were associated with a higher risk of MetSyn in HIV-infected subjects receiving HAART. We also found a strong correlation between serum RBP-4 levels and the number of components of MetSyn, in particular, its key components, including TG and waist circumference. This significant correlation was not attenuated after adjustment for age and BMI, which are known to be related to the prevalence of MetSyn.18,19 We also noted an increased prevalence of LD in HIV-infected subjects with MetSyn. These findings suggest a potential role for serum RBP-4 as a diagnostic marker for early detection of metabolic complications in HIV-infected subjects receiving HAART. To our knowledge, this is the first study to evaluate the relationship between serum RBP-4 levels and the presence of MetSyn in HIV-infected subjects. However, we did not compare serum RBP-4 levels between HIV-infected subjects receiving HAART without MetSyn and non-HIV-infected healthy individuals without MetSyn, in this study. In addition, we did not measure serum RBP-4 levels in the HIV-infected individuals who have never received HAART (treatment-naïve individuals). Therefore, there may be the possibility that neither HIV infection itself nor HAART have any impact on the association between RBP-4 and MetSyn. Further study with the aforementioned study design and a larger sample set is needed to evaluate whether serum RBP-4 levels are useful as diagnostic markers for MetSyn and/or predictive factors for the development of MetSyn or CVD in HIV-infected subjects receiving HAART, as well as to reveal the exact mechanism or causality for the relationship between RBP-4 and MetSyn in HIV-infected subjects. Because serum RBP-4 levels may be a useful marker for MetSyn and the measurement of serum RBP-4 levels is not difficult, it could allow clinicians and scientists to readily collect valuable information on metabolic complications in HIV-infected subjects receiving HAART.


 XML Download
XML Download