

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Robot-assisted laparoscopic radical prostatectomy (RLRP) has gained popularity since it was first introduced in 2001, and is widely replacing conventional open prostatectomy. RLRP entails benefits of reduced blood loss, nerve sparing, less postoperative pain, and shorter hospital stay.1,2 For optimal surgical exposure, RLRP usually requires a steep Trendelenburg position and prolonged intraperitoneal carbon dioxide (CO2) insufflations, resulting in increased intraabdominal pressure.3 CO2 insufflations during laparoscopic surgery, which causes peritoneal stretching and irritation, is known to play an important role in postoperative nausea and vomiting (PONV).4 If temporally extended, the pneumoperitoneum can also increase the risk for PONV.4 PONV causes patient discomfort and can lead to prolonged stay in the post-anesthesia care unit (PACU). Patients with PONV are also predisposed to complications of dehydration, electrolyte imbalance, aspiration pneumonia, increased wound dehiscence, delayed recovery, prolonged hospital stay, and increased medical cost.5-8 Accordingly, anesthesiologists should give attention to preventing PONV in patients undergoing RLRP, because the RLRP itself can be an important risk factor for PONV, although most patients involve fewer patient-related risk factors.5,9
Previous clinical studies suggested that total intravenous anesthesia (TIVA) with propofol significantly reduced PONV when compared to inhalation anesthetics.10,11 Furthermore, several studies recommended TIVA with propofol for anesthesia in patients at high risk for PONV.12-15 However, no studies were designed to evaluate the incidence and severity of PONV in patients undergoing RLRP at low risk for PONV.
We designed a prospective single-site, double-blinded, randomized, and parallel-arm controlled trial to investigate the effects of TIVA with propofol on PONV in patients undergoing RLRP in comparison to balanced anesthesia with desflurane. The primary endpoint was to compare the incidence and severity of PONV for 48 hours postoperatively.
MATERIALS AND METHODS
This trial was conducted at Yonsei University College of Medicine, Seoul, Korea, between November 2010 and May 2011. In addition to gaining the approval of the Institutional Review Board of Yonsei University College of Medicine (4-2010-0361) and registration with clinicaltrial.gov (Unique Identifier: NCT01402622), this study was performed in full compliance with the Declaration of Helsinki. All participants were recruited from the anesthesiology preoperative evaluation clinic and provided written informed consent. Sixty two male patients scheduled for RLRP, with an American Society of Anesthesiologists physical status of I or II, ranging in age from 50 to 70 years, were enrolled. To control the anticipated risk for PONV, we excluded patients with a history of motion sickness or PONV, antiemetic use within 24 hours before surgery, regular corticosteroid use, chemotherapy within 4 weeks or radiotherapy within 8 weeks, hepatic dysfunction, confirmed renal impairment, or obesity (body mass index >35 kg/m2). Patients were randomly allocated to either the balanced anesthesia (Des group) or TIVA (TIVA group) group by means of random numbers generated by a computer. Antiemetic prophylaxis was commonly administered in both groups. A physician of the anesthesiology preoperative evaluation clinic who was not involved in the current trial performed randomization and assignment.
All patients were premedicated intravenously with midazolam 0.05 mg/kg and glycopyrrolate 0.2 mg at 1 hour and just before the induction of anesthesia, respectively. Standard monitoring devices were applied. In the TIVA group, propofol and remifentanil were concurrently infused using a target controlled infusion (TCI) system for induction and maintenance of anesthesia. Effect site concentration was controlled using the Marsh, et al.16 and Minto, et al.17 models for propofol and remifentanil, respectively. After the loss of consciousness, intravenous rocuronium 0.6 mg/kg was administered for relaxation. After tracheal intubation, a 20-G radial artery catheter was inserted for continuous blood pressure monitoring. The effect site concentrations of propofol and remifentanil were kept within the ranges of 2-5 mcg/mL and 2-5 ng/mL, respectively. In the Des group, anesthesia was induced with propofol bolus (1.5 mg/kg) and remifentanil, and maintained with desflurane and remifentanil. Like the TIVA group, remifentanil was infused using a TCI system. The end-tidal concentration of desflurane and the effect site concentrations of remifentanil were kept within the ranges of 4-7% and 2-5 ng/mL, respectively. During the surgery, the concentrations of propofol, desflurane, and remifentanil were titrated to maintain an arterial blood pressure and heart rate within 20% of baseline values. The depth of anesthesia was monitored using a bispectral index score monitor (A-200 bispectral index score monitor, Aspect Medical System Inc., Newton, MA, USA) within the range of 40-60. Controlled ventilation was performed with 40% oxygen in air to maintain end-tidal CO2 at 35-40 mm Hg during the surgery. Body temperature was controlled to within 36-37℃ using a forced air warming system throughout the surgery. During the operation, CO2 pneumoperitoneum was induced to maintain an intraabdominal pressure of 15±5 mm Hg using the Da Vinci Robot Surgical System (Intuitive Surgical, Sunnyvale, CA, USA) in a 30° Trendelenburg position. All patients received ramosetron 0.3 mg intravenously at 20 minutes before the end of the surgery. In both groups, postoperative pain was controlled using intravenous patient controlled analgesia (PCA), consisting of fentanyl 20 mcg/kg mixed with normal saline to comprise a total volume of 100 mL, administered at a basal rate of 2 mL/hour, with a bolus dose of 0.5 mL and a 15-minute lockout time. After extubation in a fully awake status, patients were transported to the PACU.
Nausea intensity was assessed using an 11-point verbal numerical rating scale (VNRS; 0-no nausea, 10-worst and intolerable nausea). The presence of nausea was defined as VNRS ≥1. The occurrence of PONV was defined as the presence of nausea, retching or vomiting. The severity of PONV was graded according to the VNRS and the presence of retching or vomiting (mild: 1-3, moderate: 4-6, severe: 7-10 or with retching or vomiting). Postoperative pain was assessed using the visual analogue scale (VAS; 0-no pain, 100-worst and intolerable pain). An investigator who was blinded to the intraoperative management assessed the VNRS, VAS, and incidences of nausea, retching, or vomiting at four time periods (during stay in PACU, and 1-6 hours, 6-24 hours, and 24-48 hours postoperatively). Patients were asked to rate the VNRS of their most severe episode of nausea during each time period. Rescue antiemetic (ramosetron 0.3 mg) was administered intravenously for nausea >6 on VNRS and rescue analgesics (ketorolac 30 mg) for pain >4 on VAS.
Continuous variables were reported as means±SD. Dichotomous variables were presented as number of patients (percent). Between-group comparisons of continuous variables were performed by Student's t-test or Mann-Whitney U test, as appropriate. Dichotomous variables were compared using the chi-square or Fisher's exact test. In a preliminary study, 70% of patients had postoperative nausea after RLRP using the same anesthetic method as the Des group. A power estimation analysis of the preliminary study suggested that 31 patients per group would be required to obtain a power of 80%, considering a type I error of 0.05, and expecting a reduction from 70% to 35% in the incidence of postoperative nausea. All statistical analyses were performed using SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
RLRP was performed as planned in all patients and complete data sets from the 62 patients were analyzed without any missing data.
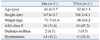
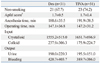
Patients' characteristics were similar between the two groups (Table 1). Preoperative and intraoperative variables associated with PONV, including Apfel score,9 anesthesia time, operating time, and fluid balances, were similar between the two groups (Table 2).
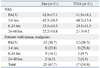
Because no significant differences were found between the groups after 6 hours postoperatively, data on postoperative nausea and vomiting were presented for three time periods (PACU, 1-6 hours, and 6-48 hours) to discriminate immediate, early and late postoperative incidences (Table 3). The overall incidence of nausea during the first 48 hours postoperatively was significantly lower in the TIVA group compared to the Des group (p=0.004). The incidences of nausea during PACU stay and at postoperative 1-6 hours were significantly lower in the TIVA group, compared to the Des group (p=0.023 and 0.001, respectively), but not significantly different at 6-48 hours postoperatively.
VNRS at PACU and 1-6 hours postoperatively was significantly lower in the TIVA group compared to the Des group (p=0.043 and 0.001, respectively). VNRS at 6-48 hours postoperatively were not significantly different between the two groups. In the Des group, retching developed in 4 and 6 patients, vomiting was reported in 1 and 3 patients, and rescue antiemetic drug was administrated in 4 and 8 patients at the PACU and postoperative 1-6 hours, respectively. However, none of the patients in the TIVA group demonstrated retching, vomiting, or rescue antiemetic requirement during the same periods (Table 3).
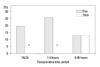
The incidence of moderate to severe PONV during the first 48 hours postoperatively was significantly lower in the TIVA group [2 (6.5%)] compared to the Des group [10 (32.3%), p=0.01], especially in the PACU [0 (0%) vs. 6 (19.4%), p=0.01) and at postoperative 1-6 hours [0 (0%) vs. 8 (25.8%), 0.002] (Fig. 1).
Pain intensity and the number of patients who required rescue analgesics were comparable between the two groups (Table 4).
DISCUSSION
In this prospective, double-blinded, randomized, and parallel-arm controlled trial, TIVA with propofol reduced not only the incidence, but also the severity of PONV when compared to balanced anesthesia with desflurane in patients at low risk of PONV immediately after RLRP.
The cause of PONV is not yet fully understood. Multiple factors, including patient-related factors, type of the surgical procedure, or choice of the anesthetics, are considered possible etiologies of PONV.12,13 Despite the fact that the patients in the Des group exhibited only one or no patient-related risk factors for PONV and all received ramosetron as prophylaxis, the incidence of PONV was 58.1%, which is much higher than the incidence of 36% after laparoscopic cholecystectomy.18 Although anesthetized with desflurane and remifentanil, the higher incidence of PONV in the Des group in our study might be attributable to the surgery (RLRP). In laparoscopic surgery, prolonged pneumoperitoneum is known to increase the risk of PONV by 60% of the baseline value for every 30 minutes of extended operating time.4,6,12 In this study, the mean operating time of RLRP was 147 min. This is much longer than the mean operating time of laparoscopic cholecystectomy, which was recently reported to be only 35 min.19 As RLRP usually requires prolonged intraperitoneal CO2 insufflations, resulting in high intraabdominal pressure, this may have contributed to the higher incidence of PONV in the Des group.
Propofol is known to exert an antiemetic effect even though the exact mechanism is still unclear. One study reported that propofol reduces PONV by blocking the 5-hydroxy-tryptamin-3 receptor of the serotonergic system,20,21 while others reported that inhibition of the chemoreceptor trigger zone and vagal nuclei, which are directly related to nausea and vomiting, is associated with the antiemetic effect of propofol.22
Several studies showed that patients administered propofol anesthesia had less PONV than those with other anesthetics. 23-25 However, one suggested that propofol anesthesia demonstrated superiority in preventing PONV only for the immediate postoperative period at the PACU.24 Tramèr, et al.26 also put the antiemetic effect of propofol in doubt, as propofol exhibited a clinically relevant effect on PONV only for short-term period. Some studies suggested that the pro-emetogenic effect of inhalation anesthetics must be considered as an important cause of early PONV within 2 hours, and the antiemetic effect of propofol may originate from a lack of such an early emetogenic effect.27,28 In our study, we found that TIVA with propofol reduced the incidence and severity of PONV at postoperative 0-6 hours, compared to balanced anesthesia with desflurane. Although the TIVA group showed lower incidences of nausea, retching, and vomiting, and less VNRS at postoperative 6-48 hours compared to the Des group, no significant difference was observed between the two anesthetic methods after postoperative 6 hours. Our results are in agreement with a recent study,29 in which TIVA with propofol was shown to exert a preventive effect on PONV at early postoperative periods (0-6 hours) compared to isoflurane. As the antiemetic effect of propofol was shown to be maintained further beyond 2 hours postoperatively in both investigations, these results could provide evidence for the early antiemetic effect of propofol. In contrast to Grundmann, et al.,30 who reported no difference in the incidences of PONV between TIVA with propofol and desflurane/N2O in patients undergoing short surgical procedures after propofol bolus induction, the incidence of PONV was significantly lower in the TIVA group compared to the Des group in our study. Therefore, much longer use of propofol with TIVA might be effective in preventing PONV for a longer period than the use of propofol for induction only.
Previous studies have recommended TIVA with propofol as the anesthetic method for patients at high risk for PONV.12,13,15 Although patients in this study involved fewer patient-related risk factors for PONV, the surgical method itself (RLRP) led to a higher incidence of PONV at the early postoperative period in the Des group, compared to the patients administered TIVA with propofol. Moreover, TIVA with propofol was shown to reduce the severity of PONV at 6 hours postoperatively. Therefore, anesthesia with TIVA along with propofol could be beneficial for preventing and mitigating PONV at early postoperative periods in patients undergoing RLRP.
The limitation of this study is that VNRS was used to assess the severity of nausea, which solely depends on the memory of the patients. Therefore, there might be bias in regards to patient's ability to recall the severity of their nausea symptoms.
In conclusion, in order to prevent PONV after RLRP in early postoperative periods, anesthesia using TIVA with propofol could suffice, regardless of patient-related risk factors.

 XML Download
XML Download