

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The diagnosis of tuberculous meningitis (TbM) is difficult because early symptoms and laboratory results from cerebrospinal fluid (CSF) are unspecific to tuberculosis and overlap with those of other chronic diseases of the central nervous system. Late diagnosis can result in a poor prognosis and even death, and a confirmative culture study for TbM requires a long time before a diagnosis can be affirmatively made. Rapid diagnosis and proper treatment is essential for TbM and a lack of confidence in test results can delay the initiation of treatment with anti-tuberculosis medication in TbM patients.1,2 In addition, most of the tests developed for the early diagnosis of TbM are not sensitive3 and cannot be used routinely.4,5
Neuron-specific enolase (NSE) is found in relatively large amounts in neurons, peripheral nervous system tissues and neuroendocrine cells, and is, therefore, one of the most often investigated biochemical markers of nervous tissue damage. Increased NSE levels in serum, CSF, or both have been reported in several neurological diseases, including status epilepticus,6 Creutzfeldt-Jakob disease,7 acute ischemic stroke,8 head injury9 and hypoxic brain injury.10 NSE can also act as a marker of neuronal damage, especially in meningitis;11 however, data for TbM is rare. The authors of the present study attempted to confirm the usefulness of NSE and to propose a cut-off value for the differential diagnosis of TbM.
MATERIALS AND METHODS
Patients
The authors retrospectively reviewed charts from January 2000 to June 2008 to determine the levels of serum and CSF NSE obtained before starting anti-Tb or anti-viral treatment. We investigated NSE routinely for evaluating central nervous system involvement. The TbM groups were subdivided into a group of patients in whom M. tuberculosis was observed by direct smear with acid fast bacillus staining or in CSF culture (confirmative TbM) or a group of patients with CSF findings of pleocytosis with lymphocytic predominance, decreased CSF (blood glucose ratio less than 0.5), elevated protein, negative gram and India ink stains, no positive bacterial or fungal cultures, and one or more of the following: dramatic responsiveness to anti-tuberculosis medication that subsided neurologic symptoms, i.e. improvement in headache, fever, ocular movement and CSF findings; chest radiography consistent with active pulmonary tuberculosis or confirmed in another organ; typical brain CT or brain MRI findings such as hydrocephalus; edema; or basal meningeal enhancement (presumptive TbM). The age and sex matched control group included tension type headache patients diagnosed with normal neurological examination, brain imaging and CSF results. Lumbar puncture was performed in patients with meningitis-like symptoms with posterior neck pain or neck stiffness, even though tension type headaches were suspected. The aseptic meningitis group included patients who had acute onset of fever, symptoms and signs of meningeal irritation and supportive CSF findings such as a mild increase in protein, normal glucose level and predominantly lymphocytic pleocytosis, no history or clinical findings of intra or extra-cranial tuberculosis, no seizure and alteration of consciousness, no organismal growth in a culture study and conversion to normal CSF upon follow up CSF test at 3 days after the first lumbar puncture. Patients with fungal and bacterial meningitis, stroke, seizure, meningoencephalitis, degenerative disease, autoimmune disease or traumatic brain damage were excluded because these conditions can increase serum and CSF NSE levels.
Serum NSE collection and quantification
All patient samples of NSE were collected intravenously upon admission. Samples were centrifuged for 30 minutes and stored at -80℃ for later analysis. The NSE sample was analyzed using an enzyme immunoassay based on the sandwich technique including the solid-phase monoclonal antibody against NSE (Cobas Core II; Roche Diagnostics, Basel, Switzerland). Hemolytic specimens were excluded because blood cell lysis influences serum NSE level.12
Data analysis
Statistical analysis was performed with PASW Statistics software, version 18 (IBM, Chicago, IL, USA). To compare variables among the TbM, aseptic meningitis and controls groups, chi-square, one-way ANOVA and Scheffe's post-hoc analyses were used. A p-value of less than 0.05 was considered significant.
To investigate predictive factors for diagnosis of TbM, binary logistic regression was performed, where variables with a p-value of less than 0.1 in univariate analysis were entered into the multivariate analysis. To analyze the sensitivity, specificity and cut-off value of CSF/serum NSE ratio, NSE related variables significant in multivariate logistic regression were used to generate receiver operating characteristic (ROC) curves. A two-tailed value of p<0.05 was considered significant.
RESULTS
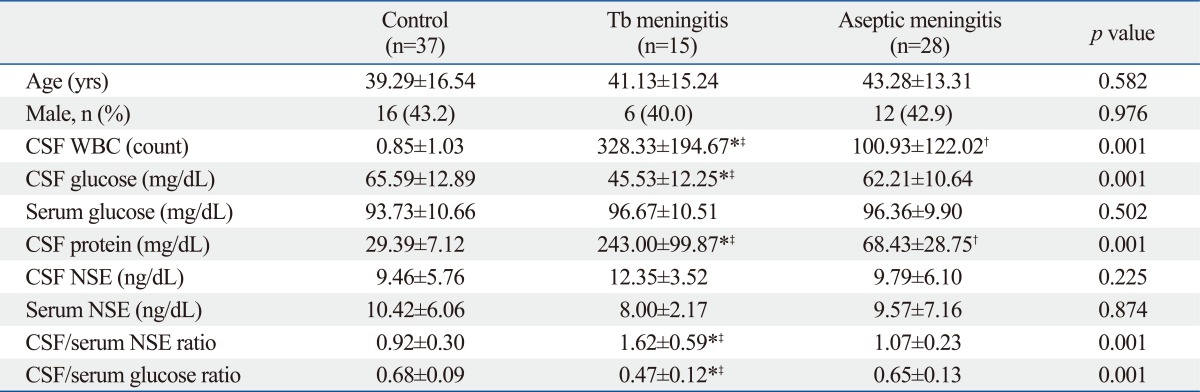
The demographic features and laboratory findings of the patient and control groups are presented in Table 1. There were no significant differences in demographic features among the three groups (Table 1). Fifteen patients were included in the TbM group, 28 in the aseptic meningitis group and 37 in the control group. The TbM group consisted of 3 patients with confirmed TbM via culture, one that was smear-positive and 11 presumptive (two patients showed dramatic responsiveness to anti-tuberculosis medication; one patient's chest radiography was consistent with active pulmonary tuberculosis; eight patients exhibited typical brain imaging findings for TbM). There were no seizures or altered mental states in TbM group and 8 patients showed basal meningeal enhancement, 3 patients showed cerebral edema, and one patient showed hydrocephalus. There were significant differences in CSF white blood cell (WBC) count, CSF glucose level, CSF protein level, CSF glucose/serum glucose ratio and CSF/serum NSE ratio (p=0.001) among the three groups.
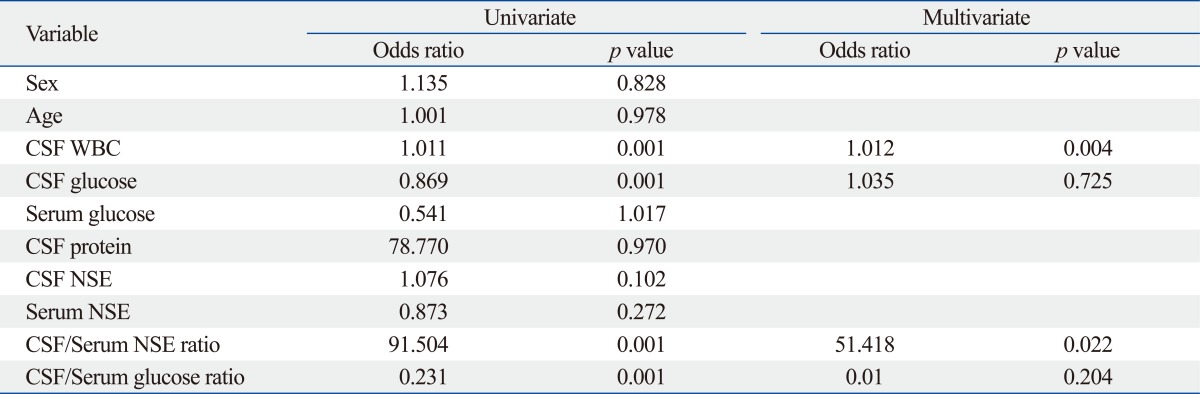
On the Scheffe's post-hoc analysis, CSF WBC count was higher in the TbM group than in the aseptic (p=0.002) and control groups (p=0.001); CSF glucose was lower in the TbM group than in the aseptic (p=0.001) and control groups (p=0.001); CSF protein was higher in the TbM group than in the aseptic (p=0.001) and control groups (p=0.001); CSF/serum NSE ratio was higher in the TbM group than in the aseptic (p=0.001) and control groups (p=0.001); and CSF/serum glucose ratio was lower in the TbM group than in the aseptic (p=0.001) and control groups (p=0.001). We performed subgroup analysis dividing the TbM group into confirmative and presumptive groups, and there were no differences in laboratory findings between the two groups (confirmative and presumptive groups) by Mann-Whitney U test. Moreover, in one-Way ANOVA and Kruskal-Wallis test, CSF WBC count, CSF glucose level, CSF protein level, CSF NSE/serum NSE ratio, and CSF glucose/serum glucose ration were significantly different among the control, aseptic and confirmative TbM group, as well as among the control, aseptic and presumptive group. In univariate logistic regression, higher CSF WBC count (p=0.001), lower CSF glucose (p=0.001), higher CSF/serum NSE ratio (p=0.001) and lower CSF/serum glucose ratio (p=0.001) were significant factors for diagnosis of TbM. In multivariate logistic regression, CSF WBC count (p=0.004) and CSF/serum NSE ratio (p=0.022) were significant prognostic factors for diagnosis of TbM (Table 2). In ROC curve, when the cut-off value of the CSF/serum NSE ratio was 1.21, the sensitivity was 86.7% and the specificity was 75.4%.
DISCUSSION
Late diagnosis and treatment of TbM leads to high mortality and poor prognosis.13,14 Therefore, rapid and accurate diagnosis is necessary for improved outcomes. Many laboratory results exist regarding diagnosis of TbM including the Ziel-Neelsen stain, CSF culture, radioactive bromide partition test,15 immunoassay,16 and latex particle agglutination.17 However, Ziel-Neelsen staining of CSF lacks sensitivity, the rate of positivity of which is approximately 40% in culture, and approximately six weeks are required to obtain a result.18,19 Our study showed lower detection rates than those of previous results18,19 and only a single positive result with Ziel-Neelsen staining (6.6%). The solid culture of M. tuberculosis from CSF is still the best confirmatory test for the diagnosis of TbM, but its sensitivity is limited. In addition, this procedure takes at least five to six weeks to demonstrate growth of M. tuberculosis. In the current study, M. tuberculosis culture was only positive in three patients (20.0%).
In our study, eight patients showed typical brain imaging findings for TbM in the presumptive group, exhibiting hydrocephalus, cerebral edema or basal meningeal enhancement on brain CT or MRI. These brain image findings suggested a high possibility of brain neuronal cell damage via vasculitis and tissue hypoxic damage. The elevation of CSF NSE in our study could be explained by the mechanism of neuron damage due to vasculitis or tissue hypoxia. Contrary to our data, a previous study20 revealed the CSF NSE level in the viral meningitis group only was higher than that in other groups, while there was no difference between the TbM and control groups. This discrepancy may be due to the small number of TbM cases in this study. In addition, high NSE level in the mumps meningitis patients increased the overall mean level.20 Moreover, in our study, we discerned that aseptic meningitis does not influence neuron damage or tissue hypoxia. Our study sample was small and there were no mumps, herpes zoster or herpes simplex infections diagnosed by PCR. In addition, there were no seizures or mental changes in the aseptic meningitis group. For these reasons, we think there was no brain damage in the aseptic meningitis group in our study.
The polymerase chain reaction (PCR) has entailed a relatively better detection rate for tuberculous agents; however, the test has not been completely validated and is often not available in developing countries where TbM is common.21,22 Although immunoassays based on CSF antigen-antibody reactions, including enzyme-linked immunosorbent assay (ELISA), have been reported with variable sensitivities and specificities16,17,23 these diagnostic methods cannot be readily used just anywhere. CSF adenosine deaminase activity (ADA) has been studied for diagnosis of TbM.24,25 CSF ADA has shown a relatively high validity, with a sensitivity ranging from 44% to 100% and a specificity of 75% to 99%. However, previous study that showed a highly reliable result with a sensitivity of 100% and specificity of 99% in only three cases.24 In addition, CSF culture for TbM requires two months to produce results. Overall, radioactive bromide partition test,15 immunoassay,16 latex particle agglutination,17 PCR, ADA and ELISA are not always accessible, and their reliabilities have not been thoroughly investigated.
In the present study, the sensitivity and specificity for CSF/serum NSE ratio were comparable with those of previous studies, especially the results of PCR, ELISA or ADA tests.15-18,23-25 Moreover, CSF and serum NSE results can be acquired more quickly and simply.
There are limitations in our study. First, our results showed a relatively low sensitivity and specificity for diagnosis of TbM. Neuron-Specific enolase estimation can non-specifically be raised in any brain disorder. Second, other chronic meningitis and partially treated bacterial meningitis cannot be differentiated by NSE, even though we excluded meningitis patients who showed suspected bacterial or other meningitis on clinical, laboratory and brain image findings. Third, the small sample size is an important limitation of our study. With only 15 cases in the disease group, the statistical reliability is weak.
In conclusion, CSF/serum NSE ratio could be a useful parameter for the early diagnosis of TbM. In addition, the authors of the present study suggest a cut-off value of 1.21 for CSF/serum NSE ratio. However, because the sensitivity and specificity were not high, clinical correlation and brain image study have to be considered for the diagnosis of TbM.
 XML Download
XML Download