

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Altered mental state occurs in many patients with serious conditions, and coma is observed in 15-20% of serious patients who require mechanical ventilation.1,2 According to a study of elderly patients in intensive care units (ICU), one-third of the patients are in a coma, and 8% of other patients fell into a coma after admission to the ICU.3 Since there are various levels of consciousness, it is too difficult to evaluate the prognosis based solely on the consciousness level. Electroencephalography (EEG) is one of the most useful methods to evaluate a patient's state of consciousness. Many EEG patterns show the cause of altered consciousness4 and can be useful for predicting a prognosis of patients.5
Some patients with altered mental state have nonconvulsive seizures (NCSz) or nonconvulsive status epilepticus (NCSE).4 Such patients have a high mortality rate, however, show good outcomes when treated with proper anti-epileptic therapy. Therefore, early detection and proper treatment of NCSE are important for good prognosis and to decrease the mortality.
We analyzed the relationship between EEG patterns and altered consciousness. In addition, we examined whether there is any relationship between EEG results and patients' prognoses.
MATERIALS AND METHODS
Subjects
We retrospectively studied 105 patients with altered mental status who underwent EEG at Gangnam Severance Hospital between January 1, 2005 and March 31, 2009. All patients were admitted to the ICU. Neurological and EEG examinations of all patients were performed by neurologists. Routine scalp EEG examinations were performed using a 17 channel analog EEG machine (Nihon-kohden, Tokyo, Japan) or a 32 channel digital machine (Grass-Telefactor, West Warwick, RI, USA). We recorded EEG for 40-50 minutes for each patient. Activation procedures, including eye opening and closure and photic stimulation, were used. Patients were excluded if they had used sedative drugs during acute phase, since it might affect EEG results. Patients were also excluded if they had a generalized convulsive status epilepticus. We retrospectively analyzed the patients' clinical records and EEG results.
Methods
We included etiologies of altered mental state such as hypoxic ischemic encephalopathy, cerebral organic lesion, metabolic encephalopathy, epilepsy, drug intoxication, and neurodegenerative disease. Cerebral organic lesions included cerebral infarction, hemorrhage, tumor, and inflammation. An organic lesion was the direct cause of acute unconsciousness of all patients. The major cause of unconsciousness was cerebral infarction, but there were many subcategories. A small number of patients whose cause of unconsciousness did not fit into categorical groups were classified as cerebral organic lesion, because sufficient samples were needed for statistical analysis. We excluded patients who received sedative drugs 934before EEG examination because such drugs could influence the patients' consciousness and their EEG results.
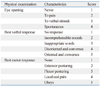
The Glasgow Coma Scale (GCS) is a reliable and objective way of assessing a person's conscious state for initial as well as subsequent assessment (Table 1). The states of consciousness were categorized into 4 degrees (coma, semicoma, stupor, drowsiness). The patient who appears to be asleep and is also incapable of being aroused by external stimuli or inner need was defined in the state of coma. In lighter stages referred to as semicoma, brainstem reflex can be elicited, and plantar reflexes may be either flexor or extensor. Patients whose GCS is 5 and less were classified as either coma or semicoma based on a chart reviews as well as physical examination. Patients' neurological outcomes were evaluated after 6-month follow-up using the Glasgow Outcome Scale (GOS). GOS is a brief descriptive outcome scale that is commonly used for investigation of early acute medical predictors of gross outcome. Grade I is a good recovery (able to return to work or school), Grade II is a moderate disability (able to live independently; unable to return to work or school), Grade III is a severe disability (able to follow commands; unable to live independently), Grade IV is a vegetative state (unable to interact with environment; unresponsive), and Grade V is death. We excluded patients who dropped out during the follow-up periods.
Patients' EEG results were divided into five classes according to the classification suggested by Scollo-Lavizzari and Bassetti.6 Grade I is dominant, normal alpha activity with theta-delta activities; Grade II is dominant theta-delta activity with still detectable normal alpha activities; Grade III is theta-delta activity without alpha activities; Grade IV is delta activity, low voltage, possibly with short isoelectric intervals or dominant, monomorphic, nonreactive alpha activity (alpha coma), or periodic generalized phenomena (spikes, sharp waves, slow waves) with very low-voltage background activity; and Grade V is very flat to isoelectric EEG (less than 10-20 mV). There can be multiple different waves in a single EEG result. A similar rhythm pattern comprising more than 50% of the result was defined as a dominant finding. EEG Grades I to III are classified according to the definition of dominant finding. If a typical wave pattern was observed in any of the EEG results, they were classified as Grade IV. Grade V EEG results showed only isoelectic activity, while none of the findings was observed in other grades.
Analysis
Spearman correlation analysis was performed on the relationship between altered mental state and prognosis and that between EEG examination results and prognosis. Linear regression analysis and equality test of correlation coefficients were conducted to determine a more decisive factor (between EEG results and GCS) in predicting the prognosis of patients. Chi-square test was conducted to compare prognoses with EEG results. Ordinary logistic regression analysis was conducted to determine whether a prognosis is correlated either with the etiologies or EEG results.
RESULTS
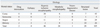
The mean age of 105 patients was 63.2±16.3 years (range: 12-89 years), and there were 64 male and 41 female patients. The most common cause of altered mental status was hypoxia which was found in 46 patients (43.8%). Metabolic causes were observed in 24 patients (22.9%), and cerebral lesions in 28 (26.7%) (Table 2). According to the GCS and chart review, 45 patients (42.9%) were in a coma, and other patients' mental statuses are summarized in Table 1. Before undergoing EEG examination, 27 patients had experienced seizures, four of whom also had a history of epilepsy.
EEG showed that three patients (2.3%) were in NCSE. Epileptiform discharges were observed in eight patients, periodic lateralized epileptiform discharges (PLEDs) in two, burst suppressions in two, triphasic waves in one, alpha coma patterns in six, and electrical silence in nine patients. EEG Grade I was shown in four patients, Grade II in 12, Grade III in 47, Grade IV in 32, and Grade V in nine. Patients' GCS scores ranged from 3 to 13, and the mean was 6.06±3.02. During the follow-up period, 29 patients (27.6%) died, and 17 of them (16.2%) did so within one month after EEG examination. Patients were evaluated 6 months after discharge from the hospital using GOS. GOS Grade I was observed in 29 patients, Grade II in 45, Grade III in 13, Grade IV in 12, and Grade V in six.
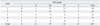
Correlation analysis was performed to determine whether the prognosis is associated with EEG and GCS results. The EEG results were well-correlated with GOS, and the Spearman correlation coefficient was -0.353 (p<0.01). GCS was associated with GOS, and the Spearman correlation coefficient was 0.464 (p<0.01) (Fig. 1). We tested the equality of population correlation coefficients by the absolute value, and found no significant difference (p=0.340). The EEG results and GCS were similarly associated with the outcome of patients. We analyzed the relationship between EEG results and prognosis, and found no uniform results showing a significant correlation between the two (p<0.05) (Table 3). Based on simple correlation analysis results, ordinary logistic regression analysis was performed to find out whether EEG results could actually predict the outcome of patients. In the ordinary logistic regression analysis, EEG grades were shown as a significant predictor only for the outcome with odds ratio (every one point of GOS) of 1.0324 (p<0.0001). We found no significant associations between the etiologies. The etiologies could not predict the outcomes of unconscious patients.
DISCUSSION
NCSz are electrographic seizures with little or no overt clinical manifestations, therefore, EEG is necessary for detection. The incidence of NCSz is 8-37% of comatose patients, and NCSE 8-19%.7,8 Such patients have a higher rate of death.4 Previous studies revealed that NCSE is not a rare condition, but less than the actual number of patients is diagnosed with NCSE, because some of the patients are in a coma. In general, EEG is not performed for all patients to confirm NCSz or NCSE.7 The level of consciousness of critically ill patients decreases without any definite cause, requiring the use of EEG. The incidence of NCSE in our study was lower than previously reporteds. Privitera, et al.9 reported that 37% of patients with altered levels of consciousness showed EEG, and clinical evidence of definite or probable NCSE by 30-45 min of routine EEG recording. Continuous EEG monitoring was applied in many other studies,4,10-12 and showed that half or more of patients had seizures, which did not appear on the routine EEG,12 another study showed a similar result with epileptiform discharges emerged in 15% of patients for the initial 30 minutes of EEG, and in about 50% of patients for one hour of EEG tracing.13 We also performed routine EEG for more than 40 minutes, and found that the incidence of NCSE was lower than other studies. It is quite possible that the low incidence of NCSE could be attributed to racial difference. Further prospective studies with a large patient series are needed to prove our suggestion about the actual incidence of NCSE.
In our study, we had a small number of NCSE patients, but none of them died. Mortality was not higher in NCSE patients in a coma than other coma patients, and it is not clear whether NCSE causes death in critically ill patients or is an indicator for the seriousness of a disease.8
Most patients who fell into a coma due to a non-traumatic cause die within one month, and survivors usually do not recover the independent mental function.14,15 As the critical care for brain damage developed, survivors often live with severe dysfunction. Some studies evaluated GCS to make the prognoses of patients with altered mental state,16,17 and results revealed that GCS is well-correlated with prognoses of patients who had fallen into a coma after cardiopulmonary resuscitation and non-traumatic causes.18-22 Our results also showed a correlation not only between the prognosis of patients with altered mental state and GCS, but also between the EEG gades and GCS.
The presence or absence of EEG activity within the theta or alpha frequency range during compressed spectral array predicts clinical outcomes.23,24 Most EEG patterns in an altered mental state were non-specific. However, some of their aspects can be used to determine the causes of an altered mental state.11 There were several point systems that classified the degree of abnormal EEG features. When determining a prognosis, it is best to relate the EEG to the entire clinical picture and to consider whether potentially reversible factors may be operative. The less ambiguous the categories, the better the inter- and intra-rater reliability.25
Some prospective studies analyzed whether EEG can predict the prognosis of patients after cardiopulmonary arrest.26 EEG results after 36 hours of monitoring were divided into five stages according to EEG wave frequency and predicted the survival possibility of patients with a precision of 98%.27 When EEGs were divided into six grades in 75 patients with cardiopulmonary arrest, a good prognosis was shown by patients with high grades and GCS of 5 or higher, and the precision of a death prediction was 90%. Patients with low EEG grades and GCS lower than 5 were considered to have a poor prognosis.28 When classifying the EEG results of 408 patients with cardiopulmonary arrest, Scollo-Lavizzari and Bassetti6 found that the higher their classes were, the higher the rates of their recovery were, and that most patients with EEG Grades IV and V died.
Our study analyzed not only patients with cardiopulmonary arrest, but also patients whose consciousness was lowered for various causes. It was reported that a low EEG grade indicates poor prognosis. In patients with GCS lower than 5, 47.5% died, and 42.5% fell into a vegetative state. In patients with GCS of 5 or higher, 46.2% showed a good prognosis and results were similar to other studies.
In general, EEG is not performed for patients with an altered mental state except who undergo neurological treatment. However, EEG findings reflect the mental status of patients, and EEG grades are correlated with the clinical prognosis of patients. It seems that more significant results can be obtained if many patients with diverse causes undergo EEG examination and monitoring.

 XML Download
XML Download