

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Aspergillosis develops in immunocompromised patients. Ureteral aspergilloma is a rare condition. We experienced a case of invasive aspergillosis arising from ureteral aspergilloma.
CASE REPORT
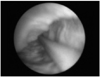
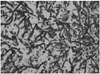
A 56-year-old man presented with complaints of right flank pain, fever, and chills for one month. He had alcoholic cirrhosis of the liver with ascites (Child C) and hepatic encephalopathy, esophageal varicosis, and diabetes. A physical examination demonstrated right flank tenderness and abdominal distension from ascites. Laboratory findings on blood samples showed a white blood cell count of 141.8×102/µL (80.9% neutrophils) and a serum creatinine of 1.12 mg/dL. Urinalysis showed the presence of red blood cells, white blood cells, urobilinogen and leukocyte esterases, but the urine culture was negative. Previous urinalysis had showed the presence of red blood cells and white blood cells, and it the earlier infection had been controlled by antibiotics. A transabdominal ultrasound image showed a 1.2 cm hyperechoic polypoid mass with a lobulated margin in the dilated renal pelvis of the right kidney. An abdominopelvic computed tomography (CT) scan showed a heterogenous attenuated lesion in the dilated right upper ureter with an enhancing wall. Ureteroscopic findings showed a 2 cm whitish mass in the edematous ureteral orifice. Another 3 cm sized, saprophytic mass was detected in the upper ureter (Fig. 1). Entire mass was removed completely with ureteroscopic forceps and an NTrap™ basket (Cook Medical, Spencer, IN). After removal of the mass, turbid urine came down from the kidney. Pathological results of the ureteral mass showed fruiting bodies and septate filaments, 5 to 10 µm thick, branching at acute angles. It was confimed as a fungal hyphe which was consistent with aspergillosis (Fig. 2). Washing cytology showed the presence of neutrophil as the dominant inflammatory cell. The patient refused antifungal pharmacotherapy and was discharged. Two months later, he visited again with right flank pain, fever, and general weakness. A follow-up CT scan showed an infarcted right kidney with multifocal necrotic lesions (Fig. 3). We also noticed an abrupt luminal obstruction of the right renal artery and thrombosis in the right renal vein. Despite treatment with broad spectrum antibiotics and the antifungal drug (amphotericin B: 50 mg/day), his condition worsened due to invasive aspergillosis. The laboratory finding on blood samples showed a white blood cell count of 173.3×102/µL, a serum creatinine of 5.96 mg/dL, a serum albumin 1.9 g/dL, a serum total bilirubin 19.31 mg/dL, and a serum direct bilirubin 13.83 mg/dL. Urinalysis showed the presence of a red blood cell, white blood cell and yeast. He was critically ill with aggravated condition of invasive aspergillosis accompanied by alcoholic cirrhosis, despite an intravenous antibiotics and anti-fungal drug. He died from sepsis and hepatorenal syndrome.
DISCUSSION
Aspergillus, a filamentous fungus, was first described in 1729 and has been implicated in several clinical manifestations. It is easily isolated from the air, soil, decaying vegetation, and even dust. Although there are more than 200 species of Aspergillus, the most common infecting species are Aspergillus fumigatus, Aspergillus flavus, and Aspergillus terreus. Aspergillosis is a common fungal infection worldwide. There are three major categories of aspergillosis: allergic disease, including allergic bronchopulmonary aspergillosis, noninvasive aspergilloma of classic fungus balls, and invasive aspergillosis.1
Invasive aspergillosis is a highly lethal infectious disease that develops in immunocompromised patients, such as those with malignancy, immunodeficiency syndrome, immunosuppressive agents, or organ transplantation. It also infects patients with alcoholism, chronic liver disease, diabetes and severe chronic obstructive pulmonary disease. Although the primary site of Aspergillus infection is the lung, spores may also infect cutaneous, naso-orbital, and genitourinary regions.2
Invasive aspergillosis has several manifestations that depend on the organs involved. It manifests in pulmonary, neurologic, cutaneous, naso-orbital, and disseminated forms. Disseminated aspergillosis has a predilection for vascular invasion, can spread hematogenously throughout the body, and can lead to death.3 Antifungal pharmacotherapy with voriconazole, echinocandins, or amphotericin B, improves the chance of survival. The drug of choice may be influenced by cost, intravenous access, drug toxicity, and patient comorbidities. The mortality rate for untreated disseminated aspergillosis is 100%.4
Aspergillosis of the urinary tract is rarely reported, but may occur from hematogenous spread, obstructive uropathy, or ascending infection.5,6 Ureteral aspergillosis may induce ureteral obstruction and hydronephrosis. Early diagnosis and treatment is challenging. Although abdominal CT scan can reveal infection, it is not a confirmative diagnostic tool.7 Urine cultures may not find Aspergillus. The fungal ball can be treated effectively by surgical resection and antifungal pharmacotherapy. Endoscopic management through either an antegrade or a retrograde approach is also effective.8 Small fungal balls can be treated with antifungal drugs before surgery.9
Initially, we did not suspect aspergilloma because of a negative urine culture and non-specific CT scan findings, however, found that the ureteral obstruction was caused by aspergillosis in the operation. We suggested a course of antifungal therapy to treat residual ureteral fungus in this immunocompromised patient. However, after removal of the fungal ball, the patient refused systemic antifungal therapy. His condition worsened, leading to invasive aspergillosis and ended into the renal infarction. He subsequently had renal infarction through vascular invasion of invasive aspergillosis and showed no response to antifungal pharmacotherapy.
His renal function deteriorated and the patient progressed to metabolic acidosis and septic shock. Our case illustrated that a ureteral obstruction due to aspergilloma can progress to invasive aspergillosis and death.

 XML Download
XML Download