

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Obesity is one of the major worldwide public health problems, affecting more than one billion people.1 For the past several decades, the prevalence of obesity in not only adults but also in children and adolescents has risen worldwide.2,3 Korea is no exception: there has been a rapid increase in obesity among children in this country. The prevalence of obesity has risen 10.5-fold for boys and 4.2-fold for girls aged 6-17 years since the 1980s.4
Regardless of age, obesity causes significant health risks. Obese children and adolescents with cardiovascular disease risk factors such as hypertension, hypertriglycemia, low high-density lipoprotein (HDL) cholesterol, high fasting glucose levels and low cardio-respiratory fitness are more likely to develop Metabolic Syndrome (MetS) as adults.5,6 Additional medical complications caused by childhood obesity include an increased risk of metabolic syndrome, whose symptoms are obesity, impaired glucose tolerance, hypertension, dyslipidemia, and/or a prothrombotic, inflammatory vascular environment, and which results in increased cardiovascular risk even in childhood.7
Because of the many different sets of criteria for MetS in both adolescents and adults,8 there have been incongruent results as to the prevalence of MetS.9,10 The most commonly used definition for adolescents is that of Cook, et al., based on The National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III). Applying the definition of NCEP ATP III, the overall prevalence of MetS among Korean adolescent aged 12-19 was reported to be 9.2% in 2001,11 which was higher than the 6.4% reported among U.S. adolescents in the National Health and Nutrition Examination Survey (NHANES) 1999-2000.6 Our study aimed first to show the linear trends of prevalence of MetS by obesity level from adolescent to adult age groups in Asia. Identifying the linear trends of MetS for adolescents and adults might allow us to see the impact of obesity on MetS for each age group and to provide tips on the time of intervention.
The purpose of this study was to estimate the prevalence of MetS in adolescents and adults and to compare the impact of obesity on MetS between adolescents and adults.
MATERIALS AND METHODS
Subjects
The data for this study came from the Third Korean National Health and Nutrition Examination Survey (KNHANES III), a national survey conducted in 2005 by the Korea Center for Disease Control and Prevention.12 KNHANES III used a stratified, multistage probability sampling design. The data were collected from adolescents aged 10 to 19 years and adults aged 20 years or more. All participants were asked to sign a written consent form. Six thousand one hundred and eighty-six people [male 2,718 (43.9%); female 3,468 (56.1%)] who 747completed the health examination questionnaire and had full data from a medical exam were chosen for this study.
Measurements
Anthropological measures such as height, body weight, and waist circumference were measured for the health examination. Height was measured to the nearest 0.1 cm on a stadiometer with the subject standing barefoot. Body weight was measured to the nearest 0.1 kg on a balanced scale while the subject wore a lightweight gown or underwear. Body mass index (BMI) (kg/m2) was calculated as weight (kg) divided by height squared (m2). Waist circumference was measured to the nearest 0.1 cm at the midpoint between the lowest rib and the uppermost lateral border of the right iliac crest. Systolic (SBP) and diastolic blood pressures (DBP) were measured with a standard mercury sphygmomanometer for each individual at a sitting position after resting for five minutes. After measuring the first blood pressure of the right upper arm, the second and third blood pressures were measured with 30 seconds intervals. The second and third readings each of SBP and DBP were recorded, and the average of each measurement was used for data analysis. Blood samples were obtained from an antecubital vein in the morning after 12 hours of fasting, and analyzed at Seoul Clinical Laboratories. Fasting serum glucose, triglycerides, total cholesterol, and HDL-cholesterol were measured by the enzyme method.
Criteria of metabolic syndrome, obesity and being overweight
We used the definition of MetS from the modified NCEP ATP III for adolescent proposed by Cook, et al.9 and the definition from NCEP ATP III for Adults developed by National Cholesterol Education Program (Table 1).13 Those with at least three abnormalities among the five components were defined as having MetS.
The criteria for the waist circumference and BMI defined as obesity in adults was taken from the criteria of the International Association for the Study of Obesity and the International Obesity Task Force, which was developed for Asian populations.14 Obesity or being overweight in adolescents were defined as ≥95th percentile BMI or as ≥85th but <95th percentiles BMI, respectively, after being adjusted for age and gender. Normal adolescents were defined as BMI<85th percentile.15 The cut-off values for waist circumference and BMI percentiles in adolescents were based on the Korea Growth Charts by gender and age developed by the Korea Center for Disease Control and Prevention in 2005.16 The cut-off points for high blood pressure were based on the systolic or diastolic blood pressure in the 90th percentile or above for age, gender, and height using the National Heart, Lung, and Blood Institutes in the US.17 The height percentile values for each child were based on Korea Growth Charts.
Statistical methods
Data were analyzed using SAS version 9.1. Sampling weights were used to estimate the representative data for Korean adolescents and adults. General and biomedical characteristics of the subjects including gender were processed by Surveymeans and Surveryfreq procedures. Continuous variables were presented as mean (standard error), and categorical variables were presented as a weighted percent (standard error). The prevalence of MetS and its components by BMI in adolescents and adults were processed using the Surveyfreq procedure, and the Chi-Square test was used to examine the linear association between obesity status and the prevalence of MetS. The Surveylogistic procedure was conducted to analyze the magnitude of association between MetS and obesity by adjusting the covariates of age, gender, smoking, alcohol drinking and physical activity. Statistical significance was estimated at alpha error 5%.
RESULTS
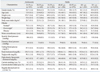
General and biochemical characteristics of the subjects were shown in Table 2. The prevalence of overweight and obese body types was 8.6% and 12.1% among adolescents, and increased to 24.7% and 31.5%, respectively, among adults aged 20 or older.
The prevalence of MetS by obesity is presented in Table 3. The prevalence of MetS was 6.4% in adolescents and 22.3% in adults. The proportion of subjects with MetS among obese adolescents (95th percentile ≤BMI) and adults (25≤BMI) were higher (35.0% and 46.9%, respectively) than among those who were overweight or had a normal BMI in both adolescents and adults. The prevalence of MetS by BMI level for both adults and adolescents was statically significant (p<0.001). For adolescents, except for the high glucose component, each component by BMI was shown to be statistically significant. The highest rates among the components of MetS among obese adolescents and adults were central obesity (60.7% for adolescents; 73.3% for adults) and low HDL (55.0% for adolescents; 65.2% for adults). Also, all components by BMI for adults were found to be statistically significant (p<0.001).
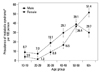
Fig. 1. showed the prevalence of MetS by gender and age group. All age groups showed a significant gender difference except for the 50-59 age group; males had a higher prevalence than females for all age groups 10-49. On the other hand, females had a higher prevalence in the 60 and above age group. There was no significant increase in MetS between the 10-19 and 20-29 age groups among males and females. A rapid increase was observed in the 30-59 age group in both genders (8.8 and 19.1 in the 30s; 16.5 and 29.7 in the 40s; 36.4 and 39.1 in the 50s for females and males, respectively). On the other hand, in the 60 or more age group the trend differed with gender; the prevalence (51.4) was still higher in female but it decreased in males (29.7).
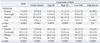
The ORs of obesity and being overweight in MetS in adolescents and adults are shown in Table 4. The ORs of obesity and being overweight with MetS compared with normal BMI in adolescents were 28.1 (95% CI 11.4-69.1) and 8.7 (95% CI 2.3-33.1), respectively. The ORs of obesity in MetS were 32.0 (95% CI 7.5-136.9), 32.2 (95% CI 12.8-80.8), 16.2 (95% CI 9.4-27.9), 7.6 (95% CI 4.7-12.2) and 9.9 (95% CI 6.8-14.6) for the 20's, 30's, 40's and 50's and the 60 and older age groups, accordingly, and the ORs of both obesity and overweight on MetS were statistically significant in each age group.
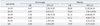
Fig. 2. presents the comparison of the prevalence of MetS in adolescents using various definitions. When the criteria by Ferranti were used, the prevalence of MetS was 13.4% (95% CI: 10.8-16.1). When we applied the new definition by the International Diabetes Federation (IDF), the most recent definition of MetS, the prevalence was 0.2% (95% CI: 0.03-1.0). The prevalence based on Cook's definition seemed to be the median as compared to the other definitions.
DISCUSSION
In this nation-wide study, the prevalence of MetS differed significantly by gender and age group. The prevalence of MetS was high in males and rapidly increased in the 30-39 year age group. Obesity was an independent risk factor for MetS in each age group. Especially, those 39 years of age or less had higher ORs than those 40 or more.
Metabolic syndrome is a risk factor of cardiovascular diseases and Type 2 diabetes. The World Health Organization in 199818 and the National Cholesterol Education Program Expert Panel III in 200113 developed definitions of MetS that have been widely used, along with the definition by the IDF. The diagnostic criteria and operational definitions are fairly broad, depending on the different organizations and authors, and reports on the prevalence of MetS have produced differing results. It is important to apply a unified definition and criteria when comparing the syndrome's prevalence among different populations in different countries. In a study of Asian North Indians, the modified NCEP ATP III criteria showed the highest occurrence of MetS in incident T2DM patients.19 In a Japanese-Brazilian study, the modified NCEP ATP III criteria was easily detected and helped health care providers screen high-risk individuals.20
For adolescents in this study, the definition of MetS by NCEP ATP III modified by Cook, et al.9 was applied for a comparison with the prevalence in adults, also defined by NCEP ATP III. The prevalence of MetS in adolescents was 6.4%, which was the same as in the US (6.4%),6 higher than that of China (3.7%),21 and lower than that of Iran (10.0%).22 The prevalence of MetS among adolescents from the KNHANES II in 2001 data was 9.2%11 which was higher than the prevalence from the present study. The lower prevalence in this study might be due to the waist circumference criteria being based on a newly developed growth curve for children in Korea. Also, there is a possibility that obesity among adolescents was overestimated in the KNHANES II data due to the use of the old version of criteria for assessing obesity among adolescents.
The prevalence of MetS showed a different pattern between males and females (Fig. 1). Females aged >50 years had a higher prevalence than males of the same age. This phenomenon was consistent with other Korean studies.23,24 Previous studies found that natural menopause is associated with elevated central obesity.23,25 Likewise, according to the KNHANES III, females have a higher prevalence of central obesity than males in the age group of 50 years or more.26 Therefore, difference in prevalence trends by gender may explain the effect of menopause on MetS in females.23,27
Fig. 2. presented the comparison of the prevalence of MetS in adolescents using different definitions. When the criteria by de Ferranti, et al.,10 another modified version of ATP III, were used, the prevalence of MetS was 13.4% (95% CI: 10.8-16.1). When adapting the definition by new IDF, the most recent definition of MetS, was applied, the prevalence was 0.2% (95% CI: 0.03-1.0). The prevalence based on the Cook's definition9 seemed to be the median as compared to the other definitions. In the 20-29 year-old group, the prevalence of MetS was 4.2 (95% CI: 2.4-6.1). As compared to the 20-29 year-old group, the prevalence of MetS among adolescents based on the Feranti definition may have been overestimated. The IDF definition for adults tends to include more people because of its lower cut off points for MetS diagnosis;28 however, reports on the prevalence of MetS based on IDF were lower in some studies and higher in others.29,30
35.0% in ≥95th percentile of BMI (obese) and 9.4% of adolescents in the ≥85th-<95th percentiles (overweight) were classified as having MetS. Other studies also have shown a similar prevalence of MetS among adolescents.5,16,17 We expected to have a lower OR of obesity in MetS among adolescents than among obese adults. The pattern of OR by age group, however, showed higher ORs among adolescents and those in their 20s and 30s than in the age groups over 40 years of age. In short, the impact of obesity on MetS among adolescents was higher than among adults over 40 years old and was similar to the impact of being obese in the 20-29 age group.
The small number of adolescents and young adults with MetS, which showed wide confidence intervals of odds ratios, may have caused some limitations to our study. One important strength of our study, however, was the use of data from the KNHANES III, which represents the general public in Korea and was collected through a well-developed study design. Although all subjects were not included due to missing responses and/or extreme outliers in their responses, the remaining subjects chosen for the study were enough to represent the general public in Korea. Our study was the first study to use the BMI and height percentile tables for Korean children developed by the Korea Center for Disease Control and the Korea Pediatric Society in 2005. The application of the NCEP ATP III definition for adults and Cook's definition for adolescents was used, and we were able to compare the prevalence of MetS and the impact of obesity on MetS between age groups.
The implication of these results might be useful and important for early detection and screening for at-risk adolescents and young adults. These high-risk individuals for MetS need to be monitored intensively once they are identified.
Further research should focus on exploring effective early screening and preventive interventions that may be used in pediatric primary care practices with young children who are overweight, obese, or at high risk for later life obesity to decrease the trajectory of child weight gain, promote healthy weight attainment, and decrease the incidence of chronic co-morbidities that are associated with overweight and obesity


 XML Download
XML Download