

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Teicoplanin, one of the glycopeptide antibiotics, is primarily active against Gram-positive microorganisms including Staphylococcus, Streptococcus, and Enterococcus species. During chemotherapy for hematologic malignancies, Gram-positive bacterial infections are a common cause of neutropenic fever in Korea as well as in western countries.1,2
Teicoplanin is known to have bi- to tri-exponential distribution features and a longer elimination half-life than vancomycin, which makes its once daily administration possible. It is also generally accepted that teicoplanin with a trough concentration (Ctrough) >10 mg/L is clinically effective; to ensure this trough concentration, a dose regimen of 6 mg/kg (400 mg) every 12 hours for 3 doses, then daily, are the minimal requirements for all patients with normal renal function, and a Ctrough of 20 mg/L should be exceeded in cases of deep-seated staphylococcal infections.3,4 Moreover, according to Harding, et al.,5 the mean trough concentration was correlated with the clinical outcome of patients with Staphylococcus aureus septicemia. MacGowan, et al.6 also demonstrated that the Ctrough >10 mg/L and Ctrough >20 mg/L of teicoplanin were related to favorable outcomes and curing of staphylococcal infections, respectively.
Dose regimens based upon trough concentrations have not considered the microorganism-specific factors. For the appropriate use of an antimicrobial agent, physicians should be aware of microorganism-specific as well as patient-specific factors. To do this, a clear relationship between pharmacokinetic (PK) and pharmacodynamic (PD) interaction of antimicrobial agents must be elucidated. The minimum inhibitory concentration (MIC) is one of the microorganism related factors that requires consideration when determining treatment doses and durations for the best clinical outcome.7 In the case of glycopeptides, the AUC24 (area under the drug concentration-time curve during 24 hr) over the MIC i.e., AUC24/MIC that associates drug exposure with the characteristics of the microorganism has recently come into use as a surrogate marker of clinical efficacy. However, there has been some debate as to the optimal level of this target for treatment using teicoplanin. Although the AUC24/MIC >125 has been regarded as a PK-PD marker that can predict clinical success with vancomycin treatment,7,8 a level of AUC24/MIC >345 have recently been recommended as the target to be attained.9,10 However, the AUC24/MIC target values for teicoplanin treatment have not been extensively studied. Therefore, clinicians have adopted those from vancomycin with the rationale that both antibiotics belong to the same glycopeptide class.
In this context, the present study was performed to assess the target attainment rate (TAR) for microorganism-nonspecific (Ctrough) and microorganism-specific (AUC24/MIC) targets during two weeks of teicoplanin administration for the treatment of S. aureus strains in Korean patients with neutropenic fever under several dose regimens.
MATERIALS AND METHODS
Teicoplanin susceptibility test of S. aureus
A total of 78 non-duplicate clinical isolates of S. aureus from patients with neutropenic fever at the Catholic Hematopoietic Stem Cell Transplantation (HSCT) Center were collected between 2005 and 2007 for this study. Most of these isolates were recovered from blood, wound, or purulent discharge. Specimens with possible contaminants or colonization were all excluded. Cation-adjusted Mueller-Hinton agar (Difco laboratories, Detroit, MI, USA) was used for tests of teicoplanin susceptibility. The method used for agar dilution was based on the protocol published by the Clinical Laboratory Standards Institute for the MIC.11 The inoculation concentration was -5×105 CFU/mL and the standard strain used for quality control was S. aureus ATCC 29213. The MICs at which 50% and 90% of the clinical isolates were inhibited were defined as MIC50 and MIC90, respectively. A frequency distribution profile was used as PD data for the clinical trial simulation. This study was approved by the Institutional Review Board of Yeouido St. Mary's Hospital, College of Medicine, The Catholic University of Korea (Protocol No. GAEUISUNG-1961, Jul/14/2003).
Population PK model and simulation
Population PK parameters of teicoplanin were adopted from a published study on neutropenic patients with hematological malignancies because the pharmacokinetic data of teicoplanin from Korean patients were not available.12 From V1 (central volume of distribution), V2 (peripheral volume of distribution), Q (distribution clearance), and CL (elimination clearance) values and their distribution, 1,000 concentration-time profiles for 14 days were generated according to several dose regimens using NONMEM (Version 6.1, Icon Development Solutions, Ellicott City, MD, USA). The dose regimens to be considered for clinical application were as follows:
400 mg single dose then, 200 mg once a day, by intravenous injection (iv)
400 mg every 12 hr for 3 doses then, 400 mg once a day, iv (standard regimen)
600 mg every 12 hr for 3 doses then, 400 mg once a day, iv
800 mg every 12 hr for 3 doses then, 400 mg once a day, iv
400 mg every 12 hr for 3 doses then, 400 mg twice a day, iv
After 1,000 virtual concentrations were obtained, for each dose scheme, the areas under the curve (AUC) were calculated from day 1 to day 14 using non-compartmental analysis with the linear trapezoidal method. Covariate effects were not considered.
Simulation of MIC distribution
Because we could not define appropriate distribution models for the histogram of MICs for S. aureus isolated from a single HSCT center, simple discrete proportions, as observed in the MIC test histograms, were used instead of assuming any distribution model for simulation of 1,000 virtual MICs. Thereafter, these 1,000 simulated MICs were randomly allocated to the above 1,000 simulated patients.
Pharmacodynamic assessment
In each of the 1,000 virtual patients, attainment of microorganism-specific and nonspecific targets (AUC24/MIC >125 [or 345], Ctrough >10 [or 20] mg/L) were determined for each dosing regimen. Thereafter, we calculated the TAR (proportions of patients showing target attainment among 1,000 virtual patients) during two week dosing periods. The AUC24/MIC >345 and AUC24/MIC >125 among the above targets were chosen to determine the relationship of the maintenance dose with a steady-state TAR, after seven days of teicoplanin administration because these targets were thought to be the surrogate marker for clinical outcomes considered with microorganism specific factors. While the AUC24/MIC >345 [or 125] was used as a target value, the logit (P=proportion of target attainment failure at day 7) was set as an outcome variable and the log (maintenance dose) values as a predictor variable because the outcome was a categorical variable. The logit (P=proportion of target attainment failure at day 7) meant the log (odds of target attainment failure) and the odds of target attainment failure was defined as P/(1-P). A logistic regression analysis was then performed using NONMEM and the logit (P) was back-transformed with the exponential and P (proportion of target attainment failure) for each dose was calculated as follows;
With this information the dose - response (TAR) relationships could be predicted. Fig. 1 summarizes the main steps taken in the present study to elucidate the dose-response relationships of teicoplanin against Staphylococcus aureus in Korean patients with neutropenic fever.
RESULTS
MIC frequency distribution
The MIC50 and MIC90 of teicoplanin for the S. aureus clinical isolates were 2 and 8 mg/L, respectively. Fig. 2 illustrates the frequency distribution of teicoplanin MICs for 78 clinical isolates of S. aureus.
Target attainment rate under several dosing scenarios
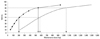
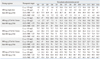
The standard dosing regimen (400 mg every 12 hr for 3 doses, then 400 mg once a day, iv) recommended by the summary in the package insert of teicoplanin for severe infections has a TAR of about 70% under steady-state (SS) conditions when Ctrough >10 mg/L and AUC24/MIC >125 were used as the therapeutic targets of teicoplanin. However, with an AUC24/MIC >345, only 33% of all patients with staphylococcal infection attained the target. When Ctrough >20 mg/L was used as a MIC-nonspecific target, less than 20% of all patients with the adopted PK parameter distributions achieved the target under SS conditions. Even though a 400 mg twice daily dose was given for maintenance, only 65% achieved a SS-TAR. Table 1 and Fig. 3 show the TARs according to several therapeutic targets with several different dosing schemes over two weeks of teicoplanin administration.
Dose-response relationships
According to several dosing scenarios the logistic regression models were analyzed with the following equation:
The dose-response (TAR) relationships observed are shown in Fig. 4. For each dosing regimen, the ED50, defined as a maintenance dose where 50% of TAR was achieved, was around 200 and 600 mg/day in the AUC24/MIC >125 and AUC24/MIC >345 targets, respectively. Since the logit (P=proportion of target attainment failure at day 7) meant the log (odds of target attainment failure) and the odds of target attainment failure was defined as P/(1-P), logit AUC24/MIC <345 or 125) equaled zero at the ED50 and ED50 for each target was thereafter calculated as follows:
When the overall clinical success was arbitrarily defined as when 80% of the patients with S. aureus infections causing neutropenia reached the target, the maintenance dose for overall clinical success was predicted to be about 540 and 1,000 mg/day in the AUC24/MIC >125 and AUC24/MIC >345 targets, respectively, and the maintenance dose for each target was obtained as follows:
DISCUSSION
According to a recent meta-analysis of 24 randomized controlled trials that compared vancomycin to teicoplanin, there were no significant differences between teicoplanin and vancomycin in terms of efficiency outcomes, such as clinical and microbiological failure rate; however, teicoplanin was associated with a lower occurrence of adverse events than vancomycin.13
Although teicoplanin has been widely used for infections associated with hematological malignancies in Korea, due to its low rate of adverse drug reactions, a population-specific optimum dose regimen has not been established with respect to its association with the PK/PD. Therefore, the goal of this study was to determine the appropriate teicoplanin-dosing strategy for adequate treatment of S. aureus in Korean patients with neutropenic fever.
To determine the effective dose regimen, validated endpoints or surrogate markers for clinical success or failure are required. In the case of teicoplanin, the trough concentration and AUC24/MIC are considered as microorganism-nonspecific and microorganism-specific markers, respectively. Moreover, the time to achieve a target value for the above marker must also be considered to associate the above markers with the clinical outcome. Because the loading dose could be readily determined from the maintenance dose using PK principles, for simplicity, the TAR with regard to the maintenance dose was studied. Both the trough concentration and AUC24/MIC are associated with the PK properties of a specific population, i.e., patients with neutropenic fever that have hematological malignancies. While the trough concentration is directly related to the dose regimen and the patient pharmacokinetics, for the AUC24/MIC, the MIC value for the microorganism has to be considered as well.
In a study reported by Whitehouse, et al.14 on teicoplanin PK in critically ill patients with renal impairment, the trough concentrations were not significantly different in the patients that were cured (mean 5.2-8.7 mg/L) and in those that failed to respond to treatment (mean 9.3-12.1 mg/L). According to Gimenez, et al.,15 eight out of 10 patients had trough concentration values below 10 mg/L at 48 hrs after a standard regimen treatment of patients with neutropenia due to underlying hematological disease. The initial inadequate concentrations during the first few days of therapy may affect the outcome of teicoplanin therapy with regard to the emergence of resistant microorganisms, and thus subtherapeutic concentrations should be avoided.16 Especially in the critically ill patient setting, loading doses of teicoplanin (6 mg/kg every 12 hrs for at least three doses) should be considered mandatory in all patients and individually optimized dose regimens optimized. In addition, drug level monitoring is important during treatment.17
Lothorary, et al.12,18 reported that patients with neutropenic fever have an increased distribution and elimination clearance without significant changes in the volume of distribution, as compared to healthy controls. Therefore, in this specific population, the trough concentration was associated with increased clearance and higher initial doses are required; administration of 6 mg/kg teicoplanin given every 12 hr for five doses ensured a mean trough serum concentration of 16.0 mg/L, with a trough concentration below 10 mg/L in 7% of patients, compared with 46% of patients on a regimen of teicoplanin given only four times during the first 48 h. According to Pea, et al.,19 to ensure early therapeutically effective trough concentrations (more than 10 mg/L at 24 h) in patients with acute leukemia, a high loading regimen (800 mg+400 mg 12 hr apart on day 1,600 mg +400 mg 12 hr apart on day 2) followed by a high maintenance regimen (400 mg every 12 hr from day 3 on) showed successful attainment of the initial target.
It is known that glycopeptide antibiotics have a time-dependent killing pattern and moderate post-antibiotic effects. Thus, the ideal dosing regimen for a glycopeptide should be designed to maximize the amount of drug received. The AUC24/MIC value could be used as the surrogate parameter associated with clinical efficacy. Unfortunately, PD data and AUC24/MIC target value are not available for teicoplanin. Therefore, the values known for the vancomycin target value were adopted. Although past recommendations had indicated that at least an AUC24/MIC >125 was necessary for vancomycin, recent studies recommend an AUC24/MIC >345 or 400.20-23 Rybak, et al.24 recommended that, for complicated infections caused by S. aureus, trough vancomycin concentrations of 15-20 mg/L should be obtained and the range should achieve an AUC/MIC >400 for most patients if the MIC is <1 mg/L. However, an AUC/MIC of >400 is not attainable with conventional doses when the MIC is more than 2 mg/L in patients with normal renal function. In that situation, alternative therapies should be considered. Therefore, it is predicted that if the present study chose an AUC24/MIC >400 as an attainable target, the TARs would show lower values than noted in the present results and larger teicoplanin doses would be needed for a favorable clinical outcome in this specific patient population with neutropenic fever. However, when the present study results were compared to clinical results from a study conducted at the same institution in which the clinical and microbiological response in febrile neutropenic patients were 53.3% and 62.5% for 200 mg/day maintenance dose regimen, the results using AUC24/MIC >125 target was more consistent with clinical results than those from the AUC24/MIC >345 target.2 Based upon this correlation between AUC24/MIC >125 target and clinical results, it might be inferred that to achieve 80% TAR, about 540 mg/day of teicoplanin would be required, and a corresponding adjustment of the standard dose regimen to 400 mg/day as a maintenance dose would be considered.
The MIC of teicoplanin for 90% of strains (MIC90) of S. aureus was reported to be below 1 mg/L3, while the MIC90 for S. aureus isolated from our HSCT center in this study was about 8-fold higher. Usual practice in Korea has been limited to low doses (400 mg single dose, then 200 mg once a day for empirical therapy; or 400 mg every 12 hrs for 3 doses, then 400 mg once a day for targeted therapy) due to the reimbursement system, which may contribute to the high MIC value for S. aureus.
Kuti, et al.25 reported that a dose of 400 mg every 24 hr achieved a trough value >10 mg/L in 46.3% of the population studied. This would be similar to a 50% likelihood of a total AUC/MIC ratio >345 at an MIC of 1 mg/L. Similarly, the 800 mg dose achieved the target trough and AUC/MIC ratios in 83% and 94% of the population, respectively. In the present study, due to the high frequency of MIC >1 mg/L, the AUC24/MIC >345 was not associated with MIC-nonspecific targets.
The results of the present study show that TARs at SS were only related to maintenance doses due to the PK properties of the PK/PD marker. With respect to the Ctrough >10 mg/L target, the standard recommended regimen, i.e., 400 mg q 12 hr iv for 3 doses then 400 mg once a day, showed that the current loading dose was insufficient to achieve SS-TAR during the early period of treatment in neutropenic patients. However, in the case of the AUC24/MIC, TAR achieved an earlier SS-TAR with the standard regimen compared to the MIC-nonspecific targets.
The logistic regression analysis for TAR of AUC24/MIC ratio >345 with log (maintenance dose), suggested a higher dose was required than in previous reports for an adequate clinical success rate in the patient population. With respect to the emergence of resistance, the MIC breakpoint or dose regimen needs to be adjusted; however, there has been no definite consensus or guidelines established to date.26
In conclusion, the current standard dose regimen (400 mg q 12 hr for 3 doses then, 400 mg once a day, iv) is predicted to be insufficient to treat S. aureus in Korean patients with neutropenic fever when the AUC24/MIC >345 was chosen as a PK/PD target to predict the clinical outcome. To assure at least an 80% TAR in this population, over 1,000 mg/day of teicoplanin as a maintenance dose is required and dose adjustment of teicoplanin would be considered. The limitations of the present study were that PK parameters from the literature were adopted instead of being based on the values of the patients in the study and the MIC values from single hospital in Korea were used. Therefore, additional well-designed prospective PK/PD outcome studies are needed to guide the optimal dosing regimens for specific patient populations.



 XML Download
XML Download