

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
High-dose chemotherapy (HDCT) and autologous hematopoietic stem cell transplantation (HSCT) are currently the modalities of choice for the treatment of children with high-risk solid tumors that respond poorly to conventional chemotherapy. While HDCT and autologous HSCT have improved the survival of these patients, significant treatment-related morbidity and mortality remain, for which infectious complications play a major role.
Invasive fungal infection is one of the most important treatment-related complications of allogeneic HSCT recipients. Various prophylactic antifungal agents are used in transplantation centers according to standard guidelines for allogeneic HSCT.1-4 However, no standard guidelines or consensus exists on the use of antifungal prophylaxis for autologous HSCT recipients, since they are generally considered to have a more rapid hematological recovery and require less severe immune suppression than allogeneic HSCT recipients. In general, routine antifungal prophylaxis has not been recommended for autologous HSCT recipients. However, studies have recommended administering antifungal prophylaxis to subpopulations of autologous recipients with underlying hematological malignancies such as lymphoma or leukemia, or those who have or will have prolonged neutropenia and mucosal damage from intense conditioning regimens or graft manipulation.5 Therefore, even in the autologous HSCT setting, patients with certain conditioning regimens with a high rate of mucositis might be susceptible to invasive fungal infection and require antifungal prophylaxis during the early post-HSCT period, until neutropenia and mucositis are resolved.
Itraconazole is an antifungal agent that belongs to the azole class and has been used as a first-line antifungal agent for the management of neutropenic fever in immunocompromised patients.6,7 However, the efficacy of prophylactic itraconazole has not yet been established for pediatric autologous HSCT recipients. In the present double-blind randomized clinical trial, the efficacy of prophylactically-administered itraconazole was prospectively evaluated in pediatric autologous HSCT recipients with high-risk solid tumors. The efficacy and safety of itraconazole prophylaxis were compared to those of empirical treatment.
MATERIALS AND METHODS
Patients
From April 2006 to March 2008, fifty-five patients with high-risk solid tumors at the Pediatric Stem Cell Transplantation Unit of Samsung Medical Center had 90 autologous HSCT episodes that were eligible for this study. The high-risk solid tumors included high-risk neuroblastoma, high-risk embryonal brain tumor, bilateral advanced retinoblastoma, and relapsed solid tumors. The Samsung Medical Center Institutional Review Board approved the protocols used for this study, and written informed consent was obtained from the parents of each patient.
Use of itraconazole and antibacterial agents for neutropenic fever
Patients were randomized in a double-blinded manner into either a prophylaxis or an empirical treatment group, and were prospectively evaluated for the safety and efficacy of itraconazole prophylaxis. In the prophylaxis group, itraconazole was given intravenously (2.5 mg/kg/dose, twice daily for the first two days followed by 2.5 mg/kg/dose once daily for the duration of treatment) after the absolute neutrophil count (ANC) fell below 0.5 × 109/L after initiation of HDCT, even in the absence of a high fever. In the empirical treatment group, a placebo was given once the ANC fell below 0.5 × 109/L after the initiation of HDCT, and itraconazole was started only when a high fever persisted for more than three days or if fever recurred despite the use of first-line antibiotics for more than three days. A placebo visibly identical to normal saline was provided by the pharmacy. Itraconazole level was not measured because the procedure was not available at our institution.
Cefepime was used as the first-line antibacterial agent, and teicoplanin and amikacin were added as second-line agents if fever persisted for three days on cefepime, or if a fever recurred despite more than three days of cefepime treatment. The antibiotic regimen was changed to imipenem and teicoplanin as third-line agents for patients who had persistent neutropenic fever for an additional three days or for recurrent fever after treatment with three antibiotics for more than three days. All antibiotics including itraconazole were discontinued after three consecutive days of no significant fever (< 37.5℃), no evidence of documented or clinically suspected infection, and an ANC exceeding 0.5 × 109/L. For microbiologically documented infections, the antibiotic regimen was altered as needed.
In all patients, chest X-rays and cultures from blood, urine, and stool specimens were performed on first fever episodes and before changing antibiotics. In some patients with prolonged fever for more than 7-10 days, additional studies such as chest or abdominal CT or ultrasound examination were performed. Tests for serum Aspergillus antigen were performed in certain patients.
Assessment of efficacy
Patients were assessed for the development of invasive fungal infections until 30 days post-transplantation or the time of discharge. Clinical parameters such as the total duration of fever and duration of antibiotic treatment were also evaluated over this period. Other parameters that could have influenced the development of infectious complications were also compared, including age, underlying disease, tumor recurrence, time from diagnosis to transplantation, type of HDCT regimen, number of transplantations (first vs. second in tandem transplantation), infused stem cell number, time to reach an ANC of 0.5 × 109/L, and duration of severe neutropenia (ANC < 0.5 × 109/L).
Assessment of safety
Adverse events were recorded until 30 days post-transplantation or the time of discharge. Data from renal and liver function tests were also analyzed. Events were classified according to the Common Toxicity Criteria grading system of the National Cancer Institute.8
Assessment of cost-effectiveness
Costs between the two groups were compared in terms of duration of hospitalization, cost of total treatment during the transplantation period, and cost of antimicrobial agents.
Statistical analyses
The Chi-square test was performed to compare the frequency of factors that were suspected to increase the risk of fungal infections. The Mann-Whitney U test was performed to compare infused stem cell numbers and hematological recovery between the two groups. The Student's t-test was performed to compare the total duration of fever and antibiotic treatment between the two groups, and to compare the duration of hospitalization and the cost of treatment. Differences in the frequencies of various toxicities between the two groups were analyzed using a Chi-square test. Multivariate analysis was also performed using linear regression analysis to examine the factors associated with duration of fever.
RESULTS
Patient characteristics
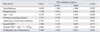
A total of 90 transplantation episodes in 55 pediatric patients met the criteria for this study. Three patients were excluded because of complications that occurred before the initiation of itraconazole or placebo treatment. In total, 87 transplantation episodes (43 in the prophylactic group and 44 in the empirical group) were included. In the empirical treatment group, one patient receiving the placebo died due to severe cyclophosphamide-related myocarditis. In the prophylaxis group, one patient who had received itraconazole for four days developed asphyxia and a severe hypoxic injury, and later died of multiorgan failure. These deaths were not considered to be associated with itraconazole treatment. Therefore, 85 episodes (42 in the prophylactic group and 43 in the empirical group) were analyzed. The two groups had similar clinical characteristics, and the clinical parameters for the risk of developing invasive fungal infection were comparable between the two groups (Table 1).
Efficacy analysis
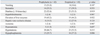
No cases of proven, probable, or possible invasive fungal infection occurred in either group. However, the duration of fever above 38℃ was significantly shorter in the prophylaxis group than in the empirical group (4.7 ± 2.4 days vs. 6.5 ± 3.5 days, p = 0.007, Fig. 1A). In addition, the number of patients who had fever for more than seven days, which were the duration of antibiotic use, and the number of patients who needed additional second-line antibiotic treatment were significantly lower in the prophylaxis group than in the empirical groups (Table 2). No significant differences in the development of documented viral or bacterial infections were observed between the two groups.
Multivariate analysis showed that prophylactic use of itraconazole was associated with shorter duration of fever, and that treatment with a thiotepa-containing regimen was associated with longer duration of fever (Table 3). Thiotepa is a well-known chemotherapeutic agent that causes severe mucositis and thus fever. A subgroup analysis of patients who were treated with a thiotepa-containing regimen showed that the prophylaxis group still had a shorter duration of fever (Fig. 1B). Another subgroup analysis of patients who did not have severe diarrhea showed that the prophylaxis group also had a shorter duration of fever (Fig. 1C).
Safety analysis
High grade toxicities (grade ≥ 3), including stomatitis, diarrhea, increased liver enzymes, hypokalemia, and hypophosphatemia, developed in more than one-third of the patients. However, no difference was observed in the development of serious adverse events between the prophylaxis group and the empirical treatment group, even though the prophylaxis group received itraconazole for a longer duration (13.9 ± 2.8 days vs. 8.9 ± 3.8 days, p < 0.001)(Table 4). In all but two HSCT episodes, patients received cefepime for neutropenic fever with no episodes of neurotoxicity.
Cost-effectiveness analysis
The duration of hospitalization for transplantation was shorter in the prophylaxis group than in the empirical group; however, this result was not significant. Similarly, the cost of total treatment during hospitalization and the cost of total antimicrobial agents were lower in the prophylaxis group than in the empirical group, but these findings were also not significant (Table 2).
DISCUSSION
The risk of invasive fungal infection after HSCT is greater in allogeneic HSCT recipients than in autologous HSCT recipients.9-19 The incidence of invasive fungal infection in pediatric allogeneic HSCT recipients is reported to be 1.3-13% for Candida infection and 3-14% for mold infection, while, the incidence is 5-6% for Candida infection and 0.3-3% mold infection in autologous HSCT recipients.17,20-25 Nationwide data of 152,231 immunocompromised children in the United States, including 822 autologous HSCT recipients, show that 0.3% of autologous HSCT recipients had invasive aspergillosis.17 Therefore, although less frequent than in allogeneic patients, serious invasive fungal infections can still occur in autologous HSCT recipients.13,19,26-29
Very limited data are available on the effects of antifungal prophylaxis in autologous HSCT recipients, particularly in pediatric recipients with high-risk sold tumors. In a meta-analysis of antifungal prophylaxis reported by Robenshtok, et al.30 antifungal prophylaxis reduced all-cause mortality, fungal-related mortality, and invasive fungal infections in allogeneic recipients. For autologous HSCT, effect estimates of antifungal prophylaxis [RR 0.27, 95% confidence interval (CI) 0.08-0.95 for all-cause mortality; RR 0.28, 95% CI 0.06-1.28 fungal-related mortality; RR 0.36, 95% CI 0.13-1.01 for invasive fungal infection] were similar to those for allogeneic HSCT recipients (RR 0.62, 95% CI 0.45-0.85 for all-cause mortality; RR 0.52, 95% CI 0.27-0.99 for fungal-related mortality; RR 0.33, 95% CI 0.18-0.63 for invasive fungal infection]. However, in this study, the samples lacked the power to reach significance, so that the data were insufficient to determine whether antifungal prophylaxis should be recommended for patients with solid tumors undergoing autologous HSCT. Therefore, the topic of whether antifungal prophylaxis should be recommended for autologous HSCT recipients is still under debate. While many transplantation centers have used antifungal prophylaxis for allogeneic HSCT recipients, no standard guidelines or consensus about the use of antifungal prophylaxis in autologous HSCT recipients have been established. In this context, we investigated the efficacy of prophylactic itraconazole by comparing with that of empirical treatment in pediatric autologous HSCT recipients with high-risk solid tumors.
Since no case of fungal infection occurred in either study group, we could not determine the efficacy of antifungal prophylaxis for the prevention of invasive fungal infection. However, the duration of fever was significantly shorter in the prophylaxis group compared to the empirical group, while no differences were observed between the two groups in the frequency of factors that might increase the chance of infection. In addition, patients in the itraconazole prophylaxis group required a shorter duration of antibacterial treatment, and fewer prophylaxis patients needed second- and third-line antibiotic regimens. These findings suggest that undiagnosed subclinical fungal infections could have occurred in many of our patients, and that the antifungal agent was beneficial for the patients in the prophylaxis group. In this way, the antifungal prophylaxis may have influenced the requirement for second- or third-line antibacterial agents.
Invasive fungal infections in autologous HSCT recipients occur most frequently during the pre-engraftment period.31 During pre-engraftment neutropenia, mucositis and the presence of indwelling central venous catheters are important risk factors. Multivariate analysis indicated that treatment with thiotepa-containing regimens and the prophylactic use of itraconazole were independent factors associated with fever duration. Since mucositis facilitates the development of fungal infection, mainly from Candida species, via damaged mucosal barriers, we expected that the benefit from antifungal prophylaxis would be greater in patients with severe mucositis than in patients without mucositis. A subgroup analysis of patients who received thiotepa and developed severe mucositis showed that the prophylaxis group had a shorter duration of fever than did the empirical treatment group. However, in patients without severe diarrhea, the prophylaxis group also had a shorter duration of fever. These findings suggest that antifungal prophylaxis could have contributed to a reduced duration of fever regardless of the severity of the gross mucositis.
A meta-analysis of randomized-controlled trials comparing fluconazole and itraconazole for antifungal prophylaxis in patients with neutropenia and hematological malignancies suggested that, even though itraconazole might be more effective than fluconazole for preventing fungal infections, its association with more adverse effects may limit its use.7 In contrast, a study that compared posaconazole and fluconazole or itraconazole prophyalxis in patients with neutropenia showed that itaconazole did not have a significantly increased frequency of serious adverse events compared to fluconazole or posaconazole.32 In the present study, no difference in serious adverse events was observed between the prophylaxis group and the empirical treatment group, even though the prophylaxis group received itracon hematopoiazole for a longer duration. Itraconazole was safely used in both groups without serious adverse effects.
One limitation of this study is that the drug levels of itraconazole were not measured. However, since all the patients received intravenous itraconazole, we assumed that the itraconazole concentration reached the therapeutic range reported in the literature, and that bioavailability was less variable than with the oral capsular form of itraconazole.33,34 A possible cefepime-associated neurotoxicity has been recognized.35-38 However, our study population showed no incidence of suspected neurotoxicity due to cefepime. Quality-adjusted life years and cost-effectiveness of transplantation are important issues when determining antifungal prophylaxis.39 Although we did not observe a significant difference in duration of hospitalization or cost-related transplantation/antimicrobial agents between the prophylaxis and empirical groups, we did observe a tendency for lower total treatment costs in the prophylaxis group than for the empirical treatment group. The issue of cost-effectiveness of antifungal prophylaxis requires further attention.
The above findings suggest that some autologous HSCT recipients might benefit from antifungal prophylaxis without increased toxicity, although the incidence of invasive fungal infection is low in autologous HSCT recipients. However, patients with prophylaxis received a longer duration of antifungal treatment than those in the empirical treatment group, so that the benefits from prophylaxis must be weighed with caution against a potential increase in the risk of drug toxicity, increased cost, and selection for resistant and rare fungal pathogens. The above factors are associated with longer use of antifungal agents, although they were not observed in this study.
In summary, this study was the first prospective double-blinded randomized trial to examine the efficacy of prophylactic antifungal use in pediatric autologous HSCT recipients with high-risk solid tumors. Although some beneficial effects, including a shorter duration of fever and reduced need for antibiotic use were observed for the prophylaxis group, this study could not definitely conclude if antifungal prophylaxis should be routinely recommended for pediatric autologous HSCT recipients with high-risk solid tumors. Further investigation with a larger cohort of patents is needed.



 XML Download
XML Download