

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Based on historical data, pneumonia has been categorized into community-acquired pneumonia (CAP) and the nosocomial pneumonia which has been further differentiated into hospital-acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP).1,2 Recently, the number of non-hospitalized patients who are in regular contact with the health care centers is increasing. And over the last several years, many investigators have documented that the pathogens coming from health care systems may be different from the pathogens seen in patients from other populations who have been admitted to the hospital from the community.3-5 Therefore, a fourth category, healthcare-associated pneumonia (HCAP), has been introduced.2,6 Previous studies have documented that compared with CAP patients, HCAP patients are often at greater risk for colonization and infection with a wider spectrum of multi-drug resistance (MDR) pathogens.5 However, HCAP patients have had a variably reported frequency of drug-resistant gram-negatives pathogens and Staphylococcus aureus.7,8
The population in South Korea is now aging very rapidly and there are about 5 million people aged 65 or older.9 Therefore, CAP is an important cause of illness, admission and death in South Korea, particularly for elderly adults.10 Furthermore, nearly 1 million of the elderly suffer from dementia, strokes or other chronic cardiovascular illnesses. Therefore, HCAP has a upward trend in an acceleration degree with the increase of health care center.
HCAP patients tend to be older than CAP patients.5-8,11,12 Because age is a well known risk factor for the poor prognosis of pneumonia and diseases in elderly patients seem to differ in microbial spectrum, it is not clear whether the poor outcome observed in HCAP patients is related to the presence of more comorbidities and old age or to a higher incidence of antibiotic-resistant bacteria and inappropriate empirical antibiotic treatment.13,14 However, epidemiological studies for HCAP in South Korea, especially in elderly patients, are limited.
The objective of this study was to determine the differences in baseline characteristics, pathogen distribution and outcomes between HCAP and CAP, especially in elderly patients, in university-affiliated hospitals in South Korea.
MATERIALS AND METHODS
Study design and setting
We conducted a retrospective observational study of patients with pneumonia older than 60 years old between January 2007 and December 2008 in Chung-Ang University Hospital and Yongsan Hospital, Seoul, Korea. Patients with HAP were excluded. We compared the baseline characteristics, comorbidities, severity, distribution of pathogen, antibiotics, and clinical outcomes between HCAP and CAP. The severity of pneumonia was evaluated using the pneumonia severity index (PSI).15 The Institutional Review Board of the Yongsan Hospital and Chung-Ang University Hospital approved this study.
Definition
The clinical diagnosis of pneumonia was based on the following criteria: 1) the presence of new cough with or without sputum production, pleuritic chest pain, dyspnea, 2) a new radiographic infiltrate compatible with pneumonia, 3) the presence of fever (> 38℃) or hypothermia(≤ 35℃), leukocytosis (> 11.0 × 109/L) or leucopenia (< 3.5 × 109/L), increased arterial-alveolar gradient.16
HCAP and CAP were defined according to American Thoracic Society (ATS)/Infectious Diseases Society of America (IDSA) guidelines.2 HCAP is defined as a patient with pneumonia and any of the following historical features; hospitalization for more than 48 hours in an acute care facility within 90 days of infection, resident of a nursing home or long-term care facility, attended a hospital or hemodialysis clinic, has received intravenous antibiotics, chemotherapy, or wound care within 30 days of infection.2
Inappropriate antibiotics were defined if the empirical antibiotics were not effective against the identified pathogens based on in vitro susceptibility test.7 Initial treatment failure was defined as death during initial treatment or change of antibiotics from initial agents to others after 48 hours due to clinical instability.11
Microbiology
Pathogens in samples obtained from sputum, tracheal aspirate, and blood were investigated. Standard serologic methods were used to determine antibodies against atypical agents such as Mycoplasma pneumonia. MDR pathogen was defined as resistance to two or more different classes of antimicrobial drugs.17
Statistical analysis
All statistical analyses were performed using Statistical Package for the Social Science ver. 12.0 (SPSS Inc, Chicago, IL, USA). Continuous variables were compared, using the Student t test for normally distributed variables and the Mann-Whitney U test for non-normally distributed variables. Univariate analysis was carried out using the Chi-square test or Fishers exact test for categorical data. p values less than 0.05 were considered significant.
RESULTS
Patient characteristics
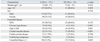
A total of 210 patients with a suspected diagnosis of pneumonia were enrolled, including 35 patients with HCAP and 175 with CAP. Baseline characteristics are described in Table 1. The median age of the patients with HCAP was 75 years old (range 61 to 91) and that of patients with CAP was 73 years old (range 60 to 97), showing no statistically significant difference between two groups (p = 0.476). Among thirty-five patients with HCAP, twenty-one patients were those hospitalized for more than 48 hours in the preceding 90 days (60.0%), eleven patients were those with residence in a nursing home or extended care facility (31.4%), four patients were those with chronic dialysis within 30 days (11.4%) and nine patients received intravenous antibiotics, chemotherapy, or wound care within 30 days of infection (25.7%). In comorbid illness, cerebrovascular diseases were significantly more frequent in HCAP than in the CAP group (43.8% vs. 14.1%; p <0.001), while chronic lung diseases (42.4% vs. 11.4%; p < 0.001) were significantly more frequent in CAP group than in the HCAP group.
Clinical, laboratory and radiographic findings at presentation
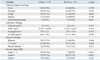
Cough was more frequent in patients with CAP, and altered mental status was more frequent in patients with HCAP. In laboratory and radiographic findings, there were no differences between two groups. Patients with HCAP were more commonly classified into moderate risk (class 4) of PSI. However, there was no difference in class 5 of PSI (Table 2).
Etiology of pneumonia
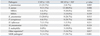
The distribution of pathogens for CAP and HCAP is listed in Table 3. A microbiologic diagnosis was established in 36.0% (63/175) of patients with CAP and in 85.7% (30/35) of patients with HCAP. Streptococcus pneumoniae was the most frequently isolated pathogens in the CAP, while Staphylococcus aureus in the HCAP. Staphylococcus aureus, Pseudomonas aeruginosa, Stenotrophomonas maltophilia and MDR pathogens were isolated more frequently in HCAP patients than in CAP patients.
Antibiotic treatment and clinical outcomes
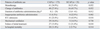
Patterns of antibiotic administration were similar in both groups, except for the fact that CAP tended to receive more combination of β-lactamase and macrolide than those with HCAP. However, initial administration rate of inappropriate antibiotics (6.3% vs. 24.2%; p = 0.002) and duration of antibiotics administration (8 days vs. 13 days; p = 0.012) were more frequent in HCAP group than CAP. HCAP group had a higher frequency than CAP group in intensive care unit (ICU) admission (42.9% vs. 23.4%, p = 0.018) and initial treatment failure (15.4% vs. 31.4%, p = 0.018). However, in-hospital mortality was not different between the two groups (Table 4).
DISCUSSION
Few studies have examined the incidence of HCAP in hospitalized patients with pneumonia, and found that the incidence of HCAP was variable between 17.3-67.4%.6-8,11 However, there was lack of data about the HCAP in South Korea. The present retrospective study showed that the incidence of HCAP was 17% in elderly patients (older than 60 years old), and that the most common pathogen in HCAP was Staphylococcus aureus. Furthermore, initial inappropriate antibiotics and initial treatment failure were more frequent in HCAP group than CAP.
Patients with HCAP could complain of atypical symptoms. The present study showed that altered mental state and lack of cough were more common in patients with HCAP. Previous studies found that cerbrovascular disease was more common in patients with HCAP.8,11 Our finding was also consistent with these studies. Our finding showed that 17 of 35 (43.8%) had a history of cerebrovascular diseases, showing a statistical difference from the patients with CAP. These patients suffered from difficulty of swallowing, and reduction of cough reflex. These patients also tended to go through a long convalescence at healthcare center and to be prone to aspiration.8 Therefore, patients with HCAP could show atypical symptoms.
Previous studies documented that HCAP is not bacteriologically similar to CAP, but HCAP patients have a variably reported frequency of drug-resistant gram-negatives pathogens and S. aureus. Kollef, et al.6 reported that S. aureus was the most common pathogen in HCAP. However, Lim and Macfarlane18 reported that the most common pathogen was S. pneumonia in both groups when compared with nursing home acquired pneumonia and CAP. Carratalà, et al.8 also reported that S. pneumonia was the most common pathogen in HCAP, although aspiration pneumonia was more common in HCAP group. Our present result showed that the most common pathogen in HCAP was S. aureus, and 9 of 12 (75%) were methicillin resistant S. aureus (MRSA). Furthermore, HCAP had a high frequency of Pseudomonas aeruginosa, Stenotrophomonas maltophilia, and MDR pathogens. In CAP, several studies demonstrated that Streptococcus pneumoniae was the most common pathogen in South Korea.19,20 Our findings in CAP were consistent with these reports. On the other hand, however, the pathogen distribution in HCAP was different, although patients with HCAP are present from in the community. This difference affects the initial inappropriate antibiotics and the failure of initial treatment. Several studies showed that HCAP patients were significantly more likely to be treated with an inappropriate antibiotic regimen.7,8,11,21-23 Our present findings are consistent with these previous studies. The ATS/IDSA guidelines suggest that HCAP should be treated as a form of HAP, using antibiotics similar to those used for patients with late-onset HAP.2 In our study, the antibiotics regimens were not different between CAP and HCAP, except for the fact that CAP tended to receive more combination of β-lactamase and macrolide than those with HCAP. This shows that HCAP has been overlooked in clinical practice. Actually, in South Korea, there are no data about HCAP and there is a lack of guideline for the treatment of HCAP. Therefore, physicians in clinical practice, tend to choose the antibiotics like to CAP patient. Considering our data, therefore, S. aureus and other drug-resistant pathogens must be considered when choosing antibiotics.
Previous investigations have shown that HCAP patients had more comorbid conditions and a higher fatality rate than CAP.1,6,8 However, our study failed to show a significant difference in mortality between CAP and HCAP. The reason for the discrepancy could be explained by pneumonia severity. Patients with HCAP were more commonly classified into PSI class 4. However, there were no differences in PSI class 5. Our study included more than 60 years old only. Age is a well known risk factor for the poor prognosis of pneumonia.14 El-Solh, et al.24 also reported that there was no difference in the outcome between those admitted from the community and those older patients who were residing in nursing homes. Therefore, CAP patients might show the same mortality rate as HCAP.
This study has several important limitations. First, the data were retrospectively collected. We did not use uniform methods for the detection of pathogens. Additionally, evaluation for atypical pathogens was inadequate because of the retrospective design. Therefore, a microbiologic diagnosis was established only in 36.0% (63/175) of patients with CAP. However, the most common pathogen in CAP was the same, compared with previous reports. Furthermore, in HCAP cases, a microbiologic diagnosis was established in 85.7% (30/35) of patients. Therefore, we can conclude that the distribution of pathogens was different between CAP and HCAP. Second, the size of the population is relatively small, therefore, our results should be interpreted with caution. Finally, the pathogens identified could be oropharyngeal colonizers and could not be definite causes of pneumonia since sputum culture could not always distinguish between colonization and true infection. Despite the limitations described above, our results nevertheless showed meaningful information about HCAP in South Korea.
In summary, the present study provides additional evidence that HCAP should be distinguished from CAP, even in elderly patients, in South Korea. Patients with HCAP were more likely to receive inappropriate initial antibiotics. Therefore, clinicians caring for patients with pneumonia who require hospital admission should be aware of the risk factors for HCAP. In addition, a proper guideline is needed for proper management of HCAP in South Korea.
 XML Download
XML Download