

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Metabolic syndrome (MetS) is characteristically defined as a clustering condition of cardiovascular risk factors including hyperglycemia, dyslipidemia, hypertension, and central obesity.1 It can not only progress to overt diabetes2-4 but also has close relationship with development and prognosis of cardiovascular disease (CVD).5 Although there have been questions as to whether MetS predicts CVD beyond its individual components,6 it is still meaningful to look into its diagnosis, management, and prevention in medicine or public health.
Despite the fact that the pathophysiology of MetS is yet not clearly known, it has been suggested that an increasingly sedentary life style and western dietary habits play a role in developing obesity and dysfunctional energy storage, which can mediate insulin resistance as well as the interaction of genetic factors, thereby contributing to recent trends.7 With the rising obese population and worldwide life expectancy, the frequency of development of MetS does not seem to diminish for the foreseeable future.8
The conception of MetS has evolved since it was first defined by Reaven in 1988 to improve the understanding of links between insulin resistance and vascular disease. Several definitions have been introduced including the World Health Organization criteria, which emphasizes hyperglycemia and insulin resistance; the National Cholesterol Education Program (NCEP) guideline, which deems all metabolic components as equally important; and the International Diabetes Federation (IDF) definition, which regards central obesity as a necessary factor (Table 1). These diverse definitions have led to substantial confusion and to an inability to compare study results. Although confusion might be caused by lower cutoff points for specific metabolic components or different criteria applied based on ethnicity, more critical issues, such as designating which components are essential, have led to large differences in prevalence.9,10 So far, the majority of research into diagnostic criteria for MetS has been done in studies that support specific criteria by comparing the prevalence11 or prospective incidence12,13 of CVD in people who satisfy each criterion. Rarely have there been studies that investigate the relationship between each component and the prevalence of CVD,14,15 and all previous studies have examined only the general population. In addition to metabolic components, however, there are many other factors that increase the risk of CVD. Thus, in order to compare the predictability of metabolic components for CVD, it would be more appropriate to study patients who have been diagnosed with MetS.
The purpose of the study was to investigate the relationship between the prevalence of CVD and each metabolic component using nationwide data for Koreans who were diagnosed with MetS according to the NCEP guidelines, in which specific factors were not weighted.
MATERIALS AND METHODS
Study population and data collection
This study was based on data obtained from the Third Korean National Health and Nutrition Examination Survey (KNHANES) of noninstitutionalized Korean civilians, which was conducted by the Korean Ministry of Health and Welfare in 2005. Detailed descriptions of the survey method have been provided elsewhere.16 Briefly, this survey was a nationwide representative study that used a stratified, multistage probability sampling design for the selection of household units. This survey was composed of four parts: health interview, health behavior, health examination, and nutrition. The surveys were performed during face-to-face interviews with the family members of randomly selected households. We performed a cross-sectional analysis of the data from the subjects who completed the health interview and health behavior survey. We excluded individuals with incomplete data for the standardized physical examination, laboratory tests, and anthropometric measures. This resulted in a final analytical sample of 1,406 subjects (587 men, 819 women) with MetS among the 5,030 participants aged 19 years or older. The presence of CVD was defined as a physician's diagnosis of any of the following on the Health Interview Survey: stroke, myocardial infarction, and angina. Smokers were defined as those who were currently smoking at the time of the survey, regardless of the number of cigarettes smoked. Participants who exercised twice a week, regardless of type or length of the exercise, were considered to partake in exercise.
Definition of the MetS
We used the revised NCEP criteria,17 which were proposed by the National Heart, Lung, and Blood Institute/American Heart Association, and require at least three of the following components: 1) abdominal obesity (waist circumference ≥ 90 cm for Asian men or ≥ 80 cm for Asian women),18 2) triglycerides ≥ 150 mg/dL or receiving drug treatment, 3) high density lipoprotein (HDL) cholesterol < 40 mg/dL for men or < 50 mg/dL for women or receiving drug treatment, 4) systolic/diastolic blood pressure ≥ 130/85 mmHg or receiving drug treatment and 5) fasting plasma glucose ≥ 100 mg/dL or receiving drug treatment. The revised NCEP criteria had recommended a lower waist circumference cutoff for Asian-Americans because Asians are predisposed to insulin resistance, MetS, and type 2 diabetes at lower waist circumferences than Caucasians.
Statistical analysis
Statistical analysis was performed using STATA SE 9 (STATA Corporation, Texas, USA) and p values of < 0.05 were considered to be statistically significant. Comparisons of the number of patients with each metabolic risk factor according to the presence of CVD were done by χ2 test, and odds ratios (OR) were calculated using multiple logistic regression analysis to evaluate the predictability of each metabolic component. All data are summarized as mean ± standard deviation or number (%).
RESULTS
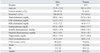
There were 1,406 subjects (587 males and 819 females) diagnosed with MetS according to the revised NCEP definition out of a total of 5,030 (2,076 males and 2,954 females). The mean age of those diagnosed was 51.8 ± 13.2 for men (28.3%) and 58.1 ± 13.2 years for women (27.7%). Information regarding various metabolic risk factors is shown in Table 2. CVD events occurred in 6.9% of men and 8.6% of women. Among these events, stroke occurred with the highest frequency for both men and women.
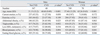
Table 3 shows differences in the percentage of CVD events based on each metabolic risk factor. The CVD group was significantly older than the non-CVD group in both men and women. In addition, there was a significant difference in high fasting glucose (FG) in men and high blood pressure (BP) and high FG in women. The percentage of current smokers or who had high triglyceride was higher in the non-CVD group; however, this was statistically insignificant. This is not irrelevant, considering standards of Korean health insurance coverage for lipid-lowering drugs and reverse causality due to cross sectional design.
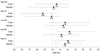
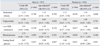
Logistic regression analysis of CVD events for each component of MetS prior to correction showed that high BP and high FG were statistically significant (OR: high BP 2.16, high FG 2.08). After adjustment for age and gender, only high FG showed significance (OR 1.81)(Fig. 1). Gender differences, presented in Table 4, show that prior to adjustment, fasting glucose in men (OR 2.67, 95% CI 1.24-5.75) and high BP (OR 2.09, 95% CI 1.10-3.96) and high FG (OR 1.84, 95% CI 1.10-3.10) in women were significant. However, after being adjusted, no significant difference was found in either men or women.
DISCUSSION
We analyzed the relationship between the prevalence of CVD and each metabolic component in a target population, which was not representative of the general population, but was made up of patients who had been diagnosed with MetS using the revised NCEP criteria. The purpose of selecting these subjects would be first to clarify the differences for each factor associated with MetS; and second, to minimize the influence of risk factors other than metabolic components that may increase the risk of CVD. In this study, when additional analysis was performed on the general population of 5,030 subjects, we found that the factors showing significant differences between the groups with and without CVD numbered three for the men (excluding lipid abnormalities) and five for women. Before adjusting for age and smoking, the OR of women with high BP was 5.19, and after adjustment it was 2.50 (not shown in table).
In the present study, we found that the only significant factor relevant to CVD prevalence was high FG. Anderson, et al.14 showed that high FG (OR = 1.23, 95% CI 1.06-1.43) and Low HDL (OR = 1.57, 95% CI 1.31-1.89) were significantly different among the individual MetS factors at risk for coronary artery disease after adjusting for age. However, secondary analysis for the risk of death or myocardial infarction showed that only high FG was significant (adjusted hazard ratio 1.46, 95% CI 1.17-1.82). Sixty-five percent of subjects had undergone coronary angiography at the start of the study because they were at high risk for coronary artery disease. More than 70% were found to have stenosis. Although this cannot be directly compared with our study, the results also show that high FG had a strong correlation with prevalence of CVD, similar to previous reports.
There is still some major controversy regarding the diagnostic criteria for MetS. One of these is regarding which criterion is the most appropriate. So far, various diagnostic criteria for MetS have been published based on the requirements of specific components. The IDF presented new diagnostic criteria that considers racial differences and also considers central obesity as a necessary component based on its strong correlation with insulin resistance and central obesity in recent publications of the pathological mechanisms of MetS.19 However, recent studies are somewhat skeptical of considering central obesity as a necessary component,20,21 and we found no difference in central obesity between individuals with and without CVD, in both men and women. The second major controversy is that there are many other factors that have a great impact on risk for CVD besides the five metabolic components of the criteria, including age.22,23 These components should also be considered in the diagnosis of MetS. In our study, the prevalence of CVD increased 1.76 times for men and 1.66 times for women with every 10 year increase in age, and this result was shown to be statistically significant (not shown in table).
In the current study, a cutoff point of 100 mg/dL for fasting blood glucose was used, which had been recommended at the 2003 American Diabetes Association Conference24 based on studies showing a high risk of developing diabetes or CVD in subjects with impaired glucose intolerance (IGT) and impaired fasting glucose (IFG), so-called prediabetes. Based on this information, a fasting blood glucose cutoff point of 100 mg/dL was proposed for the diagnostic criteria of MetS at the 2005 IDF conference. Despite the definition of MetS, significant results were observed for prediction of CVD in both men and women when the conventional cut-off point of 110 mg/dL was lowered to 100 mg/dL. This suggests that particular caution is necessary to prevent CVD in patients with high FG who have been diagnosed with MetS, at least according to the revised NCEP definition. Among the various diagnostic criteria used to diagnose MetS, the identification of insulin resistance, including IGT and IFG, as a necessary component may more appropriately support prediction of CVD.
It is already widely accepted that ethnically specific values must be applied to waist circumference (WC) cutoff points for central obesity, one of the components of MetS.25 Recently Lee, et al.26 published their research findings on the appropriate cutoff values for Koreans based on the 1998 KNHANES data. According to their study, the WC at which the risk for developing other metabolic components increased significantly compared to the general population was 90 cm for men and 85 cm for women. Their study was in accordance with the basic concept of clustering the five CVD risk factors for MetS; however, when CVD is considered as the final outcome of MetS, future studies will be needed to define the cutoff value at which the risk of CVD increases significantly.
There are two limitations to our study. First, the clarity of the cause and effect relationship is affected by the cross-sectional research design. Since the subjects had already been diagnosed with CVD, stringent blood pressure, weight, and blood sugar control were highly likely. In addition, the fact that a greater number of men without CVD events were current smokers underscores these limitations. Second, the inclusion of the clinical diagnosis of angina pectoris with CVD is ambiguous, because unlike myocardial infarction or stroke, angina pectoris can be diagnosed by symptoms alone without specific blood test results or radiographic findings.
In summary, the predictability of each component for CVD events in patients with MetS was considerably diverse, and high FG had the highest of all of them. In patients with MetS diagnosed according to the revised NCEP criteria, aggressive management should be undertaken to reduce all standard risk factors, but particular and increased attention should be paid to preventing and treating diabetes.

 XML Download
XML Download