

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cases of acupuncture-related pneumothorax are not uncommon, but those of hemopericardium are not common comparing to pneumothorax: 191 cases1 have been reported and 18 cases1 with 7 cases of cardiac tamponade,2-8 respectively. Because these complications are fatal, rapid diagnosis and treatment are very important. We report a case of hemopericardium that occurred shortly after acupuncture and showed rapid improvement after a fast diagnosis by an echocardiography and emergency intervention.
CASE REPORT
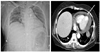
A 54-year-old woman, who was previously healthy, presented to the local hospital with dyspnea and chest discomfort 30 minutes after acupuncture. She sought the help of an acupuncturist for myalgia and dyspepsia. Acupuncture was performed to her chest (upper 5 cm, 3 cm left and right points from the mid lower xiphoid process border) and epigastric area (lower 3 cm point from the mid lower xiphoid process border) by an unauthorized acupuncturist. A right-sided pneumothorax was diagnosed on a chest X-ray, and a tube thoracostomy was performed. A hemopericardium was diagnosed on a chest CT scan after a thoracostomy (Fig. 1). She was transferred to our hospital for further treatment.
At our emergency room, the initial vital signs were: blood pressure of 109/63 mmHg, pulse rate of 80 beats/min, respiratory rate of 28 breaths/min, and body temperature of 36.2℃. Her breathing decreased bilaterally and a cardiac murmur was not present, but the heart sound was muffled. Arterial blood gas analysis showed hypoxemia and metabolic acidosis. Echocardiography demonstrated pericardial effusion without a right ventricle collapse, with a width of 2.0 cm in a subxiphoid view, 1.2 cm in a parasternal long axis view, and 1.6 cm in an apical 4 chamber view.
An emergency physician performed pericardiocentesis using a subxiphoid approach. After the drainage of 200 mL of a dark bloody effusion, the width of the effusion decreased to 0.6 cm in a subxiphoid view and she felt better (Fig. 2). Her final diagnosis was traumatic hemopericardium with right-sided pneumothorax related to acupuncture. After her admission to the general ward, the Department of Thoracic and Cardiovascular Surgery, the hemopericardium decreased without further surgical interventions. Although a pericardial drain catheter was removed 2 days after the admission following a repeated echocardiography, air leakage on the thoracostomy lasted 6 days. Finally she was discharged 6 days later without any complications.
DISCUSSION
Acupuncture is an ancient Asian system of healing and is now one of the most popular complementary therapies in Asia and other developed countries.9,10 It is a relatively safe procedure, with rates of serious adverse effects estimated to be 0.05 per 10,000 treatments, or about 0.55 per 10,000 patients undergoing acupuncture treatment.1 However, rare but potentially fatal complications can be grouped by: trauma, infection, and miscellaneous events. In the first group, pneumothorax is most common, with injuries to the central nervous system, blood vessels, and pericardium, in order of frequency. For infections, hepatitis B is the most common, with others including auricular chondritis, endocarditis, and septicemia. The miscellaneous group includes collapse, seizures, exacerbation of asthma.1 Five cases of acupuncture-related fatalities have been reported, including 2 with cardiac tamponade, 2 of Staphylococcal septicemia, and 1 from bilateral tension pneumothoraces.11 Therefore, physicians should recall these complications in patients who recently received acupuncture.
Kirchgatterer, et al.8 reported a case of cardiac tamponade that occurred shortly after acupuncture. In our case, the acupuncture points on her chest corresponded to conception vessel point 17 (upper 5 cm from the mid lower xiphoid process border) and, kidney point 22 (upper 5 cm, 3 cm left and right points from the mid lower xiphoid process border) respectively, and the epigastric area corresponded to stomach point 14 (lower 3 cm point from the mid lower xiphoid process border).12 Her vital signs were relatively stable, so her diagnosis was hemopericardium rather than cardiac tamponade. However, these 2 entities differ only in whether the heart is under elevated intra-pericardial pressure that compromises diastolic filling and systolic stroke volume, leading to profound circulatory collapse and shock.13 Here, our case was at high risk for converting to cardiac tamponade, which was the rationale for rapid echocardiography and pericardiocentesis, allowing the emergency physician to stabilize the patient.
Hemopericardium is a rare but potentially fatal complication if cardiac tamponade or shock develops, and may be associated with myocardial perforation that requires surgery. Therefore, emergency physicians should be able to appropriately diagnose (with echocardiography) and manage it (with pericardiocentesis).

 XML Download
XML Download