

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Many studies have shown that people on vegetarian diets have lower risks of ischemic heart disease mortality1-4 and even lower overall mortality rates.1,3 A vegetarian diet lowers blood pressure, serum total, and low density lipoprotein (LDL) cholesterol levels, and also improves endothelial function and insulin sensitivity, and thus reduces the risk of atherosclerosis.5-11
There are still some conflicting facts about the benefits of a vegetarian diet. For example, serum homocysteine has been reported to be higher in vegetarians than in omnivores.7,12 Homocysteine stimulates vascular smooth muscle cells to proliferate and synthesize collagen; it also affects endothelial cell function and adversely affects anticoagulation, which may result in atherosclerosis.13
Chronic inflammation is an essential feature of the atherosclerotic process. High-sensitivity C-reactive protein (hs-CRP), a very important inflammatory marker, has been reported to be a strong independent risk factor for atherosclerosis and a cardiovascular prognosis.14,15 Some studies16 showed lower hs-CRP in vegetarians than omnivores. Other studies7,17 failed to demonstrate that.
Lipoprotein-associated phospholipase A2 (Lp-PLA2), an enzyme mainly produced by monocytes/macrophages, generates potent proinflammatory products. In one study, elevated levels of Lp-PLA2 appeared to predict future coronary events in apparently healthy middle-aged men with moderately elevated total cholesterol levels, independent of hs-CRP.18 This suggests that the cardiovascular outcome predictive effect of Lp-PLA2 and CRP may be additive.18
The status of Lp-PLA2-associated inflammation in vegetarians has not been studied. Thus, we designed a cross-section study enrolling a larger number of subjects, to compare the differences in inflammation markers in addition to conventional risk factors between vegetarians and omnivores by examining hs-CRP and Lp-PLA2 levels. To eliminate any gender bias on inflammation status, we enrolled only females in this study.
MATERIALS AND METHODS
All of the subjects were adult females (more than 20 years old) who had undergone a general health examination at the Buddhist Dalin Tzu-Chi General Hospital, Chia-Yi, Taiwan, from Jan 1, 2006 to Dec 31, 2006. All of the subjects filled out questionnaires regarding their dietary preferences and past medical history. Exclusion criteria include a history of smoking, diabetes, dyslipidemia, hypertension, cerebrovascular disease, chronic gingivitis, connective tissue disease such as systemic lupus erythematosus or rheumatoid arthritis, diagnosis of a coronary artery disease, or a fever or another infectious disease within 3 weeks prior to the start of the study. Those who fit the above criteria but not on a regular vegetarian diet at least one year before inclusion were enrolled into the omnivore group. Patients who had been on an ovo-lactovegetarian diet for at least 1 year before inclusion were enrolled into the vegetarian group.
Informed consent forms were obtained from all subjects and the study protocol was approved by the research committee and the institutional review board (IRB) of The Buddhist Dalin Tzu-Chi General Hospital (B09404004).
After an overnight fast for at least 12 hours, venous blood samples were obtained from all subjects. Each patient age, weight, height, heart rate, and blood pressure were recorded before blood withdrawal on the day of study inclusion. The fasting blood samples were tested for Lp-PLA2, hs-CRP, glucose, cholesterol, triacylglycerol, high density lipoprotein (HDL) cholesterol, LDL cholesterol, uric acid and homocysteine levels, and white blood cell (WBC) counts were recorded. Frozen serum samples were used for analyzing Lp-PLA2, hs-CRP, and homocysteine. Serum Lp-PLA2 activity was analyzed by dynamic assay with a platelet-activating factor acetylhydrolase assay kit in a unit of µmol/min/mL (Cayman Chemical Company, Ann Arbor, MI, USA). Samples were centrifuged with a Micron centrifugal filter device (YM-30, Millipore, Billerica, MA, USA) under a centrifugal force of 14,000 g and temperature controlled at 4℃, to reach a cut-off molecular weight of 30,000 Daltons. hs-CRP was measured with an enzyme-linked immunosorbent assay (ELISA) based on purified protein and polyclonal anti-C-reactive protein antibodies with a unit of mg/L (Cobas Integra 800 system, Roche Diagnostics GmbH, Mannheim, Germany). Homocysteine levels were measured using an immunoassay method in a unit of µmol/L (FPIA assay, AXSYM system, Abbott Laboratories, Chicago, IL, USA).
Statistical analysis
For basic comparisons, the two groups characteristics were primarily examined by independent t-tests. Furthermore, based on the two hypotheses specified for the effects of a vegetarian diet on the inflammation factors of Lp-PLA2 and CRP, we applied linear regressions to the influencing factors for exposure to a vegetarian diet. B values with 95% confidence intervals were estimated for the effects of predicting factors. Separately, Lp-PLA2 and CRP were treated as dependent variables in univariate and multivariate analyses. In multivariate analyses, age and body mass index (BMI) were considered as potential confounders. However, in the case of secondary or intermediate associations within the causal relationship between dietary habit and these two inflammation markers, variables of basic characteristics that were not clearly independent influencing factors were excluded from the final model of multivariate analyses. SPSS 13.0 for Windows (SPSS Inc, Chicago, IL, USA) was utilized to perform all the statistical analyses and the significance level (a value) was set at 0.05.
RESULTS
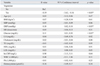
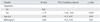
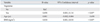
A total of 363 subjects (190 omnivores, 173 vegetarians) were involved in the analysis. Their average age was 51.9 years old (SD: 9.9 years old), and all were female. Table 1 presents the basic characteristics of each group by independent t-tests. Remarkable discrepancies for age, levels of Lp-PLA2, glucose, cholesterol, triglyceride, HDL cholesterol, LDL cholesterol, and homocysteine were detected between the two groups (p values < 0.05 or 0.01). However, basic comparisons showed no significant differences for BMI, blood pressure, heart rate, uric acid, WBC, and platelet counts. It was noteworthy that the level of CRP reached borderline statistical significance between these two groups (p = 0.05). As to the results of linear regressions on Lp-PLA2, vegetarianism had significant effects on changes on Lp-PLA2 levels on univariate analyses (Table 2). In multivariate analyses, after adjusting for age and BMI as potential confounders, vegetarianism remained a significant factor influencing the Lp-PLA2 level [B value: - 1.79, 95% confidence interval (CI): - 3.58, - 0.01; p < 0.05]. A vegetarian diet decreased Lp-PLA2 levels remarkably (Table 3). Meanwhile, because of the overall low levels of CRP among healthy subjects, the estimated changes influenced by predicting factors were tiny. Thus, we applied three digits after the decimal point. In univariate (Table 4) or multivariate (Table 5) analyses, significant positive correlation to CRP levels with vegetarianism and BMI were detected (B values for vegetarianism and BMI, separately: 0.058 and 0.010, 95% CIs: 0.001, 0.114 and 0.001, 0.018; both p values < 0.05).
DISCUSSION
Our current study demonstrated that as a new inflammation marker, serum Lp-PLA2 activity is lower in apparently healthy Taiwanese vegetarians than in omnivores. Elevated Lp-PLA2 has been proven to be an independent risk factor for inflammation, was additive to hs-CPR as a predictor of cardiovascular events18,19 and a risk factor for a new or recurrent ischemic stroke.20,21 This provided the basis that Taiwanese vegetarian diets might have protective effects on cardiovascular disease and ischemic stroke via the mechanism of lower Lp-PLA2 levels in vegetarians.
However, our results also demonstrated a lower serum hs-CRP level in omnivores than in vegetarians. This result is different from Szeto report,16 which showed a lower serum hs-CRP in apparently healthy Hong Kong vegetarians than in omnivores. It is different from our previous study, too.7 Our previous study showed a borderline lower serum hs-CRP in vegetarians but there are many study limitations in it. As we know, gender and smoking influenced the serum hs-CRP level significantly.22,23 In our previous study, there are more males and smokers in the omnivore group that can influence the statistical power of difference of hs-CRP between both groups. Actually, it failed to demonstrate a significant difference if male and female samples were analyzed separately. Also, the case number of our previous study is small. So, we conducted the present study with more subjects and only female nonsmokers were enrolled. We believe that our present study is better controlled and more reliable than our previous one. There are several possible explanations for lower Lp-PLA2 and higher hs-CRP in Taiwanese female vegetarians. Firstly, there are large variations of hs-CRP levels which makes statistical analysis difficult (as evidenced by standard deviation greater than mean in both our current study and Szeto report). Secondly, Lp-PLA2 appeared to be a specific marker of vascular inflammation, whereas hs-CRP is a circulating marker influenced by chronic systemic inflammation and obesity.24-26 Thirdly, it might be due to the geographic differences in vegetarian diets. Most western vegetarians include fresh vegetables and fruits as their main source of nutrition and energy, based on health benefits of the foods. In contrast, most Taiwanese vegetarians choose a vegetarian diet because of their Buddhist religion, which teaches a policy of "no killing" Buddhists in Taiwan have a dietary pattern similar to that of most Taiwanese in terms of meal patterns and cooking methods, except that they do not include any meat, fish, or poultry in their meals. The Taiwanese vegetarian diet includes a large intake of soybean products, which are the major substitute for animal products.27 In comparison to western vegetarians, Taiwanese vegetarians consume fewer fresh vegetables and usually cook their vegetables in oil. They also consume many deep-fried and refined soybean and grain products, which probably contain many more oxidative groups, and more oil and even trans fatty acids since trans fatty acids are mainly produced during oil hardening in food processing.28 Studies have confirmed that a diet and a cooking pattern that includes processed, fried, and refined foods, such as meats, grains, and beans, are associated with an elevation of inflammation markers, such as hs-CRP, adhesion molecules, and impaired endothelial function.29,30 Consuming foods containing more trans fatty acids will also result in higher serum inflammation markers, adhesion molecules, and impaired endothelial function.31 Further study with detailed food item questionnaires might serve to elucidate the exact mechanism.
As the Atherosclerosis Risk in Communities (ARIC) Study showed, there was no correlation between Lp-PLA2 and hs-CRP.19 According to the comments of Zalewski and Macphee,24 circulating Lp-PLA2 levels are dependent on the level of its carrier, LDL cholesterol, and CRP and Lp-PLA2 do not correlate because they probably reflect disparate inflammatory pathways.
Ridker, et al.15 demonstrated that hs-CRP was the strongest univariate predictor of future cardiovascular events (relative risk, 4.4), followed by the ratio of total cholesterol to HDL-C, total cholesterol, LDL cholesterol, and homocysteine (relative risk, 2) in a prospective case-control study of 28,263 healthy postmenopausal women followed for more than 3 years. Our study demonstrated that Taiwanese vegetarians have lower Lp-PLA2, total cholesterol, HDL cholesterol, and LDL cholesterol, but higher hs-CRP, homocysteine, and triacylglycerol. Since each of these risk factors carries different relative risk ratios, the net effect on cardiovascular protection is difficult to estimate. Long-term follow-up on this group of subjects is warranted and interventions to modify these risk profiles should be studied.


 XML Download
XML Download