

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Arthritis is a chronic disease induced by inflammation of joints. Arthritis involves destruction of cartilage which allows joints to move smoothly and absorbs pressure on the joint, thus resulting in stiffness, pain and swelling of the joints involved. Arthritis arises in various forms such as osteoarthritis, gout, rheumatoid arthritis, psoriatic arthritis, and etc. Among them, osteoarthritis is the most common. As average life expectancy has become extended, more people are vulnerable to chronic arthritis and, particularly, osteoarthritis. Although arthritis is not a primary cause of death, physical limitation, loss of ability, pain, and depression caused by chronic arthritis not only affects patients' lives but also influences the people around them. As the underlying cause of arthritis cannot usually be cured, the goal of treatment is to reduce pain.1 Thus, management of arthritic pain is most important in patients with chronic arthritis.
Acupuncture has traditionally been used in oriental medicine for the management of diseases and pain. Today, since acupuncture was proposed by a National Institutes of Health (NIH) consensus as a therapeutic intervention of complementary medicine (NIH, 1997), acupuncture efficacy has become more accepted in the western world.
Since acupuncture therapy is claimed to be effective in many medical fields, including acute pain, many investigators have attempted to explain the mechanism of acupuncture in many diverse ways. Although several studies have suggested the effectiveness of acupuncture analgesia of pain in animal models and although acupuncture analgesia is widely used in pain clinics, the results of controlled clinical studies are still inconsistent.2,3 Nowadays, there are two different approaches to acupuncture therapy, which are manual acupuncture and electroacupuncture (EA). EA combines the therapeutic effects of traditional manual acupuncture and transcutaneous electric nerve stimulation.4 In contrast to manual acupuncture, EA can be more standardized for frequency, voltage, and wave form. Moreover, some studies have suggested that EA has more analgesic effects than manual acupuncture.5 Several animal studies have shown that EA is effective against chronic inflammatory pain and ankle sprains.6,7 Also, our past study showed that EA is very effective against arthritic pain induced by the injection of carrageenan into knee joint cavities of rats.8
The aim of this study was to investigate what kinds of neurotransmitters are related with the analgesic effects of EA, using behavioral tests9 in an arthritic pain model of rats.
MATERIALS AND METHODS
Subjects
Experiments were performed on adult male Sprague-Dawley rats (250-350 gm, Daehan Biolink Co. LTD., Eumseong, Korea). Animals were housed in groups in plastic cages with soft bedding under a 12/12 h reversed light-dark cycle (light cycle: 8:00 AM-8:00 PM). Temperature (22±2℃) and humidity (50±10%) were controlled constantly. Food and water were available ad libitum. The care and use of laboratory animals in this experiment were based on the Guidelines and Regulations for Use and Care of Animals at Yonsei University.
Induction of arthritis
A standardized model for the induction of inflammatory arthritis was produced by injecting 2% carrageenan (50µL, suspended in sterile saline; Type IV lambda-carrageenan, Sigma, St. Louis, MO, USA) into the knee joint cavity of the left hind leg of the rat under halothane (1-2 vol %) anesthesia.
Weight-bearing behavioral tests
To estimate the level of pain in the arthritic knee, behavioral tests were performed starting from 4 h after the injection of carrageenan. To examine the effects of acupuncture or EA on weight-bearing force, acupuncture or EA was applied to an acupoint for 30 min under halothane anesthesia. Weight-bearing force measurements were repeated every 30 min following the termination of manual acupuncture and EA.
A special testing device causing minimal restraint of the rats was used to measure the weight bearing of the foot. This apparatus was composed of a starting box, a path, and an arrival box. The path of the apparatus was constructed in such a way that, while a rat was walking through it, the weight load on a given leg of the animal could be monitored at a maximum of four different spots along the path. The floor of the path consisted of eight acrylic plates (length: 5×10 cm) attached to load cells (Dana load cell LTD, Seoul, Korea). These plates were lined up in two rows of four. The sidewalls of the path were built with two movable acrylic plates so that the width of the path could be adjusted according to the size and walking pattern of the animal. This adjustment prevented the rat from stepping on the plates on the contralateral side. Arrival boxes were made with translucent and black acrylic plates. The starting box was illuminated with a bright light. The output of each load cell was fed to an amplifier (Neuropack 8 MEB-4200K, Nihon Kohden Co., Tokyo, Japan). The amplified signals were sent to a personal computer via an analog-digital converter (1401 Plus, CED, Cambrige, UK) and plotted as a time-weight curve using software (Spike 2, CED, Cambrige, UK). This test was initiated by placing the rat in the starting box. As the animal walked through the path between the starting and arrival boxes, the investigator identified the plates on which the rat stepped with the paw of interest.5,9
Acupoints and frequency of EA
For the main study of the analgesic mechanism of EA in the arthritic pain model of rats by carrageenan injection, a preliminary study was conducted in order to determine the most effective acupoints among four and the appropriate frequencies among low and high frequency EA.
To see what kinds of acupoint were most effective, 120 rats were examined in six groups according to acupuncture location: control group (no manual acupuncture stimulation, n=20), sham group (acupuncture on a sham-acupoint, n=20), as well as Zusanli (n=20), Yinlingquan (n=20), Hegu (n=20), and Taichong (n=20) acupoint groups. As the control group, in accordance with many previous acupuncture studies, acupuncture was applied to the respective acupoints of interest without manipulation rather than non-application to the acupuncture points.10 As for the sham group, lipid tissue located along the border of the body trunk at the thigh on the contralateral side was selected as a sham-acupoint. The needle was inserted at the sham-acupoint with the same manipulation as for the four other acupoints as follows: the stainless acupuncture needle was inserted vertically through the skin to a depth of about 5 mm, and then rotated manually right and left three times per second for each 30 min stimulation period.
In order to find out the differences of analgesic effects of EA according to low and high frequencies on weight-bearing force, 68 rats were examined in four groups: control group (n=17), sham group (n=17), low frequency stimulation of 2 Hz (n=17) and high frequency stimulation of 100 Hz (n=17). The low frequency group and the high frequency group received EA stimulation upon the needle inserted at the Zusanli and the Yinlingquan acupoint. The control group received no electrical stimulation upon insertion of the acupuncture needle. The sham group received EA stimulation upon the needle inserted at the sham acupoint.
Electroacupuncture
EA was applied to two acupuncture points for 30 min under halothane anesthesia. Two strainless steel acupuncture needles (size: 0.3 mm in diameter and 30 mm in length) were inserted into specific points, the Zusanli and the Yinlingquan acupoints at a depth of 5 mm, and electrical stimulations of 100 Hz frequency for 30 min were applied by a Stimulus Isolator A385 (World Precision Instruments, Sarasota, FL, USA) equipped with the Pulsemaster A300 (World Precision Instruments, Sarasota, FL, USA). For the electrical stimulation of 100 Hz, the pulse duration was 0.2 ms and the intensity was 2 mA for 30 min as a bipolar square wave current output. Weight-bearing force was measured repeatedly following the termination of EA.
Study groups
To estimate the analgesic mechanism of EA, 100 rats were divided into 6 groups according to respective receptor antagonists: control (n=17), EA (n=17), opioid (n=17), adrenergic group (n=17), serotonin (n=16) and dopamine (n=16).
The control group comprised only inflammatory arthritis induced pain. The EA group received EA without a receptor antagonist. For opioid, adrenergic, serotonin and dopamine groups, we injected opioid antagonist (naloxone; 1 mg/kg), adrenergic antagonist (yohimbine; 2 mg/kg), serotonin antagonist (ondansetron; 0.5 mg/kg) and dopamine antagonist (metoclopropamide; 0.5 mg/kg) intraperitoneally before stimulation with EA, respectively.
Statistical analysis
Data were presented as mean±standard error of the mean. Statistical tests were done using a one-way repeated measures analysis of variance followed by a Dunnett's (2-sided) post hoc multiple comparison at each time point. A p value of less than 0.05 was considered statistically significant.
RESULTS
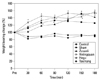
Four acupuncture points, the Zusanli, Yinlingquan, Hegu and Taichong showed similar effects for reducing arthritic pain induced by the injection of carrageenan according to weight-bearing behavioral tests. The sham point group showed no reduction in arthritic pain (Fig. 1).
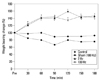
The weight-bearing force was greatly improved from 60 min to 180 min after EA compared to the control group. Frequencies of 2 Hz and 100 Hz seem to have similar effects. The responses of sham acupoint group and the control group were comparable (Fig. 2).
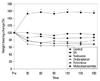
As shown in Fig. 3, in the opioid receptor antagonist group, adrenergic receptor antagonist group, serotonin receptor antagonist group, dopamine receptor antagonist group and control group, weight-bearing force decreased significantly from 30 min to 180 min after EA in comparison with EA group.
DISCUSSION
In this study, EA attenuated arthritic pain induced by carrageenan injection and the analgesic effects of EA were related to opioid, adrenergic, serotonin, and dopamine receptors.
The analgesic effect of acupuncture is a complicated neuronal process mediated by many different neurotransmitters and modulators. Many signaling molecules such as opioid peptides, serotonin, noradrenalin, dopamine, cholecystokinin octapeptide, glutamate, γ-amino-butyric acid and other bioactive substances may be involved in acupuncture analgesia. Also, many brain regions are related with opioid peptides during acupuncture. The analgesic effect of acupuncture is decreased at the supraspinal level when opioid receptor antagonists are given.11 Naloxone reversed the analgesic effect of electrical stimulation by antagonizing µ-receptors, as well as, weakly, κ-, δ- receptors. This result is consistent with the Zhang, et al. paper in which µ-, δ- receptors were related to analgesia for both 2 and 100 Hz EA in rats with inflammatory pain.12 Naloxone has already been known to block EA-induced antinociception as a result of many studies, although there are conflicting reports in human subjects. The analgesic effect of EA is largely decreased by blocking the opioid receptors in periaqueductal grey (PAG) matter with naloxone or antibodies against µ- or δ-receptors.11 The microinjection of the mixed peptidase inhibitors of amastatin, captopril and phosphoramidon into the PAG prevents hydrolysis of an enzyme-induced degradation of endogenous opioid peptides, potentiating the effects of acupuncture analgesia.13 In the current study, EA induced analgesic effect was also blocked by naloxone.
Serotonin and its receptors in the CNS are related to the modulation of nociceptors.14 An electrophysiological study reported serotonin receptor subtype antagonists are involved in EA-induced inhibition of acute nociceptive responses provoked by stimulating the tooth pulp of rabbits.15 However, there are some other compelling data. The blocking of serotonin receptors by serotonin synthesis inhibitors induced inhibition of acupuncture analgesia.10 Respectively, serotonin receptor degradation by pargyline, an amonoamineoxidase inhibitor, induced potentiation of acupuncture analgesia.16 In the current study, ondansetron, a 5-hydroxytrptamine3 (5-HT3) receptor antagonist, showed blockade of EA induced analgesic effect. These data shows that 5-HT3 receptor subtypes are important in EA analgesia in arthritic pain.
Noradrenalin plays a different role at spinal and supraspinal levels. The analgesic effects of EA are blocked by administering the precursor of noradrenalin, whereas it is potentiated by administering intrathecally.17 The analgesic effects of EA are significantly inhibited by injecting α2 receptor antagonist, yohimbine, intrathecally, but it was not inhibited by α1 receptor antagonist, prazosin, in a neuropathic pain model of rats.18 In another one of our experiments, in an arthritic pain model, the analgesic effects of EA also were blocked by yohimbine.
Some reports revealed that dopamine receptor antagonists potentiated EA analgesia.19 Dopamine receptors can be grouped into two main classes, D1-like and D2-like receptors. The main distinction between the two classes is that D1-like receptors activate adenyl cyclase, where D2-like receptors inhibit adenyl cyclase. In addition, D1 receptor antagonists increase upregulated opioid receptors in many brain regions. It shows that D1 receptors may be associated with potentiating EA analgesia.20 King, et al.21 showed that D2 receptor activation may oppose opioid analgesia. In our current study, the D2 antagonist metoclopramide reduced the analgesic effects of EA in an arthritic pain model. These somewhat conflicting results may be related to differences in the route of drug administration, receptor subtype selectivity and differences in the experimental pain model.
There are various results supporting that different frequencies in EA analgesia seem to be associated to different opioid subtypes.22,23 The administration of various specific opioid antagonists intrathecally showed that 2 and 100 Hz EA-induced analgesic effects were related to µ-/δ-, and κ-receptors, respectively. These results suggest that low frequency EA is related to µ-/δ- receptors and high-frequency EA are related to κ-receptors. This might suggest that 2 Hz EA has better pain relieving effects by producing endomorphin.24 In pathological conditions such as inflammatory pain, both 2 and 100 Hz EA-induced analgesia are related to only µ-/δ-receptors, not κ-receptors.25
In the present study, acupuncture applied to four acupoints, Zusanli, Yinlingquan, Hegu and Taichong showed similar effects on reducing arthritic pain induced by the injection of carrageenan. Therefore, we selected the two acupoints of Zusanli and Yinlingquan, which were equally effective acupuncture points, for EA study. Following EA of low frequency (2 Hz) and high frequency (100 Hz) stimulations, weight-bearing behavior was improved by EA in comparison with the control group, and there were no differences in response between the low frequency (2 Hz) and high frequency (100 Hz) stimulations. These results are different from the studies by Han, et al.11 These different results may come from various stimulation parameters such as different durations, frequencies and intensities of biphasic square pulses.
As far as we know, this is the first study to investigate the analgesic mechanism of EA in the aspect of several neurotransmitters, simultaneously. In the present study, we were able to verify that the analgesic mechanism of EA is related with opioid, adrenergic, serotonergic and dopaminergic systems, which agrees with previous studies. However, our results also showed that one of the receptor antagonists related to opioid, adrenergic, serotonergic and dopaminergic system abolished the analgesic effect of EA on the same plane as the control group. Thus, all of these mechanism may be closely connected with each other and facilitate the analgesic effect of EA. Additionally, well designed studies are necessary to investigate the relation of opioid, adrenergic, serotonergic and dopaminergic systems in the analgesic mechanism of EA.
In summary, EA attenuated arthritic pain induced by carrageenan injection. The analgesic effects of EA are related to opioid, adrenergic serotonin, and dopamine receptors in an arthritic pain model of rats.
 XML Download
XML Download