

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Systemic lupus erythematosus (SLE) is an autoimmune disorder with multiorgan involvement; it is characterized by the production of numerous autoantibodies.1,2 Although the pathogenesis of SLE remains unclear, autoantibodies against autoantigen, the deposition of immune complexes, and activation of the classical pathway complement system seem to be consequences of immune dysregulation.2,3 Abnormal immune responses involve innate and adaptive immune systems. These mechanisms-including hyperactive memory B cells and plasma cells, abnormal T cell activity, monocyte abnormalities, and immunoregulation-play important roles in the development of SLE.1,2,4-6 In patients with SLE, hyperactive B cells are triggered by an autoantigen or external antigen, to produce numerous autoantibodies that appear to have pathogenic consequences.7 These autoantibodies can induce damage to targeted organs and structures, including the skin, lung, brain, blood vessels, heart, kidneys, and joints.
Previous studies describe many new biomarkers for the survey of SLE; these potential lupus biomarkers can be used to survey susceptibility, diagnosis, disease activity, and specific organ involvement.8 The novel biomarkers to evaluate disease activity include serum cytokine, soluble cytokine receptor, soluble cell surface molecules (CD27, CD154 and BAFF), endothelial activation markers (sVCAM, sICAM and thrombomodulin), and cell markers (CD27high plasma cells and erythrocyte-C4d).8,9 Traditional biomarkers for the survey of disease activity include anti-dsDNA antibodies and serum complement levels (C3 and C4). However, a persistently high level of anti-dsDNA antibodies or a low level of complement (C3 and C4) is found in some patients with SLE. Therefore, traditional biomarkers are not always adequate in evaluating disease activity. A potential biomarker is required to survey disease activity.
Previous studies have proposed that the frequency of CD27high plasma cells is high in SLE patients, and that this metric is useful in evaluating disease activity with a significant correlation with the systemic lupus erythematosus disease activity index (SLEDAI) and autoantibodies.10,11 However, the percentage of circulating CD27high plasma cells is also increased in non-SLE patients with bacterial infection.12 Distinguishing active lupus from infection is traditionally difficult. Elevated C-reactive protein (CRP) levels over 5 mg/dL suggest the presence of infection.13,14 Our study aims to evaluate the percentage of circulating CD27high plasma cells from the peripheral blood in the SLE patient, either with or without infection.
MATERIALS AND METHODS
Study participants
All study participants were 18 years of age or above, and each provided written informed consent. None of the patients were excluded from participation on the basis of sex or ethnicity. This study was approved by the Tri-Service General Hospital Institutional Review Board (Grant no: 098-05-084) based on the declaration of Helsinki.
SLE patients
We analyzed 59 patients (52 women and 7 men) with SLE, all of whom fulfilled the 1982 revised criteria of the American College of Rheumatology, after informed consent was obtained. Disease activity was evaluated in each patient according to the SLEDAI. In laboratory studies, the following characteristics were investigated in the patients with SLE: CRP, blood urea nitrogen, creatinine, white blood cell count, haemoglobulin, platelet, anti-dsDNA, anticardiolipin IgG/IgM, anti-Sm, anti-Ro, anti-La, anti-RNP, rheumatoid factor, and C3 and C4. The flare-up of SLE was defined as the elevation over 3 points in SLEDAI (compared with the patient's previous SLEDAI) without evidence of infection.
Non-SLE patients with bacterial infections
A total of eight patients (1 woman and 7 men) with acute bacterial infection were treated with antibiotics therapy, and blood samples were collected during the hospital course. These infections included pneumonia, cellulitis, urinary tract infection, and acute cholecystitis. Different pathogens were growth from their blood culture.
Healthy controls
The control group consisted of 26 healthy donors (18 women and 8 men). These participants were required to complete a brief questionnaire regarding previous or current medical conditions.
Flow cytometric analysis
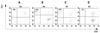
All SLE patients with or without infection and non-SLE patients with infection were monitored for their plasma cell number in peripheral blood during their hospital stay. In the SLE patient with infection, after the antibiotics or conservative treatment, the percentage of CD27high plasma cell was checked again 1 to 2 months later. Briefly, 100 µL of EDTA anti-coagulated whole blood was incubated with 20 µL fluorescein isothiocyanate (FITC)-labeled anti-CD19 and 20 µL peridinin chlorophyll protein (Per CP)-labeled anti-CD20, in combination with 20 µL phycoerythrin (PE)-labeled anti-CD27. Tubes were incubated for 20 min at room temperature before lysing solution was added. Erythrocytes were lysed with lysing solution for 10 min in the dark. Blood samples were washed with phosphate-buffered saline and analyzed on a FACS-track cytometer (Becton Dickinson). Lymphocytes were gated on the basis of forward (FSC) and side scatter (SSC). A live gate was set on the CD19+ cell population, and then we evaluated the expression of CD27 and CD20. Frequencies of CD20-CD27+ plasma cells were analyzed and calculated on the same day, using CellQuest software (Becton Dickinson, San Jose, CA, USA).
Statistical analysis
SPSS version 15.0 software (SPSS Inc., Chicago, IL, USA) was used to perform the statistical analyses in our study. Differences between median values of defined patient groups were compared using the nonparametric Mann-Whitney U test. A Spearman's rank correlation was applied, to detect correlations among different study parameters. Any p value less than 0.05 was considered statistically significant.
RESULTS
Characteristics of the four study groups
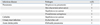
The study population consisted of 36 SLE patients without infection, 23 SLE patients with infection, eight non-SLE patients with infection, and 26 healthy controls. Among the patients with SLE, 36 patients (33 women and 3 men, mean age 38.3 ± 2.6 years) without infection did not receive any antibiotic therapy, and 23 patients (19 women and 4 men, mean age 39.3 ± 3.4 years) with evidence of viral or bacterial infection received antibiotic therapy (Table 1). In the group of non-SLE patients with infection, the bacterial pathogens are shown in Table 2. General data vis-à-vis the SLE patients of this study are shown in Table 3. SLE patients without infection had significantly higher anti-dsDNA and SLEDAI values and lower CRP and C4 values, compared to SLE patients with viral or bacterial infections. However, the other parameter cannot distinguish lupus flares and infection in SLE patients.
Frequencies of peripheral CD27high plasma cells in controls, SLE patients, and non-SLE patients with infection
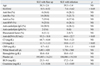
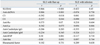
The frequency of peripheral CD27high plasma cells increased in patients of SLE without infection, SLE with infection, and non-SLE with infection, compared to healthy donors (p < 0.05). There was a significant difference of percentage in circulating CD27high plasma cells, between the SLE patients with infection and those without infection (p < 0.05). The mean percentage of circulating CD27high plasma cells was higher in the patients of SLE with infection and in the group of non-SLE with infection, and there was no significant difference between these two groups (Fig. 1). There was no significant difference between SLE patients with bacterial and viral infection (41.3 ± 7.6 vs. 47.4 ± 11.8, p = 0.548). After antibiotic therapy, the percentage of CD27high plasma cells decreased significantly in the group of SLE patients with infection (43.1 ± 6.3 decreased to 14.1 ± 1.2, p < 0.05). The mean percentage of CD27high plasma cells and CRP levels of the study group is shown in Table 4. There was a significant correlation between the percentage of peripheral CD27high plasma cells and disease activity, including SLEDAI (r = 0.866, p < 0.001), anti-dsDNA (r = 0.886, p < 0.001), C3 (r = - 0.392, p = 0.018), and C4 (r = - 0.337, p = 0.044) in the group of SLE without infection; however, there was no statistical correlation with anti-Ro, anti-La, anticardiolipin IgG/IgM, anti-RNP, anti-Sm, or RF. In the SLE patients with infection, there was no correlation between SLE disease activity and circulating CD27high plasma cells percentage, by SLEDAI or these autoantibodies (Table 5) (Fig. 2).
DISCUSSION
In humans, B cells are important to the immune system, as they produce antibodies, act as antigen-presenting cells, produce cytokines, and interact with T cells to regulate immunity-related activities.2,15 There are many regulatory mechanisms-including apoptosis, receptor editing, anergy, and clonal ignorance-underpinning B cell tolerance in healthy individuals.16-18 The loss of this tolerance may induce autoreactive B cell processes, in turn possibly incurring an autoimmune disorder. In SLE, multiple internal or external factors increase B cell reactivity, so that it can directly result in the production of pathologic autoantibodies and in end-organ damage. There are generally a large number of antibodies from the SLE patient's blood that counter self-antigens. Plasma cells containing surface markers of CD19+CD20- prodigiously secrete antibodies.11 The CD27 molecule belongs to the tumor necrosis factor receptor family and is expressed on T and B cells.11,19 CD27+ B cells are quickly activated to produce a higher level of immunoglobulin in comparison to CD27- B cells.19
Previous studies show that the expansion of CD27high plasma cells is associated with the serological presence of particular autoantibodies, including anti-dsDNA, anti-Ro, anti-La, anti-Sm, and anti-histone antibodies.10-12 In our data, circulating CD27high plasma cells seem to be important for the survey of disease activity in SLE patients without infection, because there is a significant correlation between the frequency of CD27high plasma cells in peripheral blood and disease activity (i.e., SLEDAI, anti-dsDNA, C3 and C4 level, Table 5). However, we cannot use these parameters to evaluate disease activity in SLE patients with infection, due to the fact there is no correlation with disease activity (Table 5).
In SLE patients with or without infection, a significantly increased percentage of CD27high plasma cells from the peripheral blood can be found from our data (but a significantly higher percentage of CD27high plasma cells in SLE patients with infection), when compared to healthy controls (Fig. 2). Non-SLE patients with infection also have a higher percentage of CD27high plasma cells. Infection is an important issue in SLE patients, because it is one of the most frequent causes of death among afflicted individuals.20 CRP is a traditional serological parameter used to distinguish a lupus flare-up from infection.13,14 However, no elevated level of CRP was found in patients with SLE, and the CRP level can be elevated in a lupus flare-up without infection.21,22 For this reason, CRP is not always a good parameter to evaluate SLE patients with or without infection. Novel parameters to differentiate infectious disease from exacerbation in lupus patients include low soluble Fc gamma receptor III; elevated granulocyte colony-stimulating factor; and elevations in sCD14, sICAM-1, or sE-selectin.23,24 In our data, there was no significant difference between SLE patients with infection and non-SLE patients with infection, in terms of the expansion of peripheral CD27high plasma cells. Infection is associated with immune hyperactivation caused by a triggering of external antigens and immune responses of SLE with flare-up are activated by autoantigens. Under either of these two conditions, hyperactive CD27high plasma cells increase in number. Infection should be considered another cause of increase in CD27high plasma cells.12 Plasma cells play a major role to produce antibody by homing to the bone marrow.18 During acute inflammation or infection, transiently elevation of plasma cells can be found. Therefore, the percentage of CD27high plasma cells can not be used to differentiate SLE patients with infection or non-SLE patients with infection. From our data, there were increasing plasma cell numbers in both infection and SLE flares; however, an increased percentage of CD27high plasma cells was found in the infection compared with SLE flares. The mechanism was still unclear.
Because of their long-term use of immunosuppressive therapy and persistent hypocomplementaemia, patients with SLE are at higher risk of contracting common and opportunistic infections, compared to the general population.25,26 If SLE patients hold the baseline data of the percentage of circulating CD27high plasma cells, we can evaluate whether a SLE patient is in an infectious state or not. Higher percentages of CD27high plasma cells are found among SLE patients with infection, and lower percentages of CD27high plasma cells (though higher than that in controls) are more prevalent in SLE patients with active disease. In SLE patients with infection, the percentage of CD27high plasma cells decreased significantly following adequate antibiotics therapy (Fig. 3).
Various microorganisms-including bacterial, viral, fungal, and protozoa infections-are major causes of morbidity and mortality in SLE patients with infection.20,27,28 Timely antibiotic therapy is required for SLE patients with infection, but adequate immunosuppression is required for the control of SLE with flare-up. The percentage of CD27high plasma cells provides clues for decision-making vis-à-vis appropriate therapy, when active lupus cannot be clearly distinguished from infection.
In summary, the percentage of CD27high plasma cells from peripheral blood is a good biomarker for evaluating disease activity in SLE patients who do not have infection, and it can also serve as a potential parameter for distinguishing a lupus flare-up from infection.




 XML Download
XML Download