

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Asthma is a chronic inflammatory disorder of the airways characterized by variable airflow obstruction and bronchial hyperresponsiveness.1,2 The pathogenesis and etiology of asthma are very complex and not fully understood, although an interaction of multiple genetic loci and a variety of environmental factors have been suggested as important determinants.3-6 Among them, the promising candidate gene is the cystic fibrosis transmembrane conductance regulator (CFTR) gene that is located on chromosome 7q31.2 (http://www.ncbi.nlm.nih.gov/sites/entrez?db=gene).
Mutations in the CFTR gene result in abnormal epithelial ion and water transport and may subsequently incur disturbances in airway mucociliary clearance.7 There are more than 1600 CFTR sequence variations registered in the CF mutation database (http://www.genet.sickkids.on.ca/cftr). However, the majority of mutations have been identified in Caucasians, and furthermore, the spectrum of mutations and genetic polymorphism has not been well described in Asian populations. In Korea, the presentation of classical classic cystic fibrosis (CF) is extremely rare and there are a number of reports regarding this subject.8-10 A few study show that some polymorphisms and mutations of the CFTR gene are associated with respiratory and pancreatic diseases in the Korean population.11,12
The purpose of this study was to evaluate the possible effect of the CFTR gene on susceptibility to asthma in Korean children.
MATERIALS AND METHODS
Subjects
48 subjects with and without asthma were recruited from Severance Hospital at Yonsei University for this study, comprised of fifty-seven boys and thirty-nine girls.
Asthma diagnosis was made in accordance with the American Thoracic Society (ATS). In short, current asthma was defined as recurrent wheezing or coughing in the absence of a cold in the preceding 12 months with a physician's diagnosis, and bronchial hyperresponsiveness upon methacholine challenge (PC20 ≤ 16 mg/mL) or at least 12% reversibility of forced expiratory volume in 1 s (FEV1) after inhalation of β2 agonist.13,14 Atopy was defined as a positive skin test to more than one extract of the common local aeroallergens, and non-atopy was defined as a negative skin test and serum IgE concentration less than 100 IU/mL. All subjects were enrolled before the administration of oral or inhaled corticosteroids. Patients treated with systemic corticosteroids due to asthma exacerbation in the preceding 6 months were excluded from this study.
Non-asthma subjects were age-matched to healthy children who visited the hospital for general health workups who had no history of wheezing, recurrent or chronic diseases, infection during the preceding 2 weeks, or hypersensitivity to methacholine. Non-asthma subjects also had negative results on the skin prick test for allergens and did not take any medications.14 All subjects did not have any other disease history including pancreatic diseases. Written consent was obtained from all participants before enrollment in the study, which had been previously approved by the Severance Hospital Institutional Review Board.
Genotyping
Whole blood was obtained from each subject and genomic DNA was extracted by using the QIAmp DNA blood Mini kit (QIAGEN, Hilden, Germany) as decribed.15 The genotyping was analyzed by a single base primer extension assay using a SNaPShot assay kit according to the manufacturer's protocols (ABI, Foster City, CA, USA), and polymorphisms in the IVS8 TGn and Tn microsatellites were analyzed by bi-directional nucleotide sequencing. Briefly, the genomic DNA region containing both of the single nucleotide polymorphism (SNP) was amplified with PCR reaction. Each PCR reaction contained: 10.0 ng of DNA, 1X PCR Buffer, 0.125 units of AmpliTaq Gold DNA polymerase (ABI), 3.0 mM MgCl2, 0.25 mM of each dNTP, and 0.5 pmole of each primer in 10 µL reaction volume. Reactions were incubated at 95℃ for 10 min, then cycled 30 times at (95℃ for 30 s, 60℃ for 1 min, 72℃, for 1 min) followed by 72℃ for 5 min.
After amplification, the PCR products were treated with 1 unit each of shrimp alkaline phosphatase (SAP) (Roche) and exonuclease I (USB Corporation) at 37℃ for 60 min and 72℃ for 15 min to purify the amplified products. One microliter of the purified amplification products was added to a SNaPshot Multiplex Ready reaction mixture containing 0.15 pmoles of genotyping primer. The primer extension reaction was carried out for 25 cycles of 96℃ for 10 s, 50℃ for 5 s, and 60℃ for 30 s. The reaction products were treated with 1 unit of SAP at 37℃ for 1 h and 72℃ for 15 min to remove excess fluorescent dye terminators. One microliter of the final reaction samples containing the extension products was added to 9 microliters of Hi-Di formamide (ABI). The mixture was incubated at 95℃ for 5 min, followed by 5 min on ice and then analyzed by electrophoresis in ABI Prism 3730 DNA analyzer. Results were analyzed using Gene Mapper software (ABI).
Statistical analysis
Statistical analyses were performed using SPSS 11.5 (SPSS Inc., Chicago, IL, USA). Genotype frequency comparisons between asthma and non-asthma groups were performed by chi-square test. Fisher's exact test was used if expected cell frequencies were lower than 5. Genotype frequencies at each SNP were tested for Hardy-Weinberg equilibrium. Haplotypes were assembled by using the software based on the Bayesian algorithm (Haplotyper2). All p values were based on two-sided comparisons and p values of less than 0.05 were considered to indicate statistical significance.
RESULTS
Subjects
The clinical characteristics of the 48 asthma and 48 non-asthma subjects are presented in Table 1. There were no statistical differences in demographic data such as age and sex between the two groups. However, subjects with asthma were significantly associated with lower lung function (p < 0.05). In addition, there were significant differences in total eosinophil counts, total IgE, and serum eosinophil cationic protein (ECP) with atopy-related parameters between the asthma and non-asthma group (p < 0.01).
Genotype frequencies in asthma and non-asthma groups
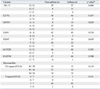
To investigate the association between CFTR genetic variations and asthma, a case-control study was performed using samples from 98 subjects as detailed in Materials and Methods. We genotyped the 14 mutations identified in Korea as summarized in Table 2.9-11 Diallelic loci were analyzed by automated DNA screening (SNaPshot; Applied Biosystems Inc.), and the TGn, Tn numbers were identified by bi-directional nucleotide sequencing. Among the 14 mutations, there are no mutant variants in Q98R, I125T, A309, Q220X, and Q1291X loci in our sample and the genotype frequencies of the remaining variants are listed in Table 3. There were no significant differences in genotype and allele frequencies of the 9 polymorphisms observed between the non-asthma and asthma groups.
Haplotype patterns and their disease associations
Since multiple alleles were analyzed in our study, a haplotype-based approach was applied to find the disease-associated CFTR variations. The Haplotype program based on the Bayesian algorithm was used and Haplotypes were assembled using the genotype data obtained from the 98 tested samples.16 Nine loci consisting of 7 diallelic variants and two microsatellites of IVS8 TGn and Tn were analyzed. Since the program accepts only diallelic data, IVS8 TGn, TG10, and TG11 were considered as wild-type (WT), and TG12 or TG13 were regarded as mutant. For IVS8 Tn, T5 was considered mutant and other alleles were applied as WT.
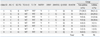
After 100 rounds of interactions, 8 haplotypes were assembled and their identification (ID) numbers were assigned according to the total sample frequencies (Table 4). Major haplotypes showing over 1% frequency in both groups are presented in this table. Differences between non-asthma and asthma groups were analyzed by the chi-square analysis. However, no significant differences were found in haplotype frequencies between the two groups.
DISCUSSION
This is the first study to investigate the association between CFTR mutations and asthma in Korean children, and no significant association was found in our pilot study. However, the association between CFTR mutations and asthma is controversial. Mennie, et al.17 did not find any association between the CFTR gene mutations and asthma in a British population. The lack of significant association between CF heterozygosity and asthma found in the present study is also supported by studies from the French,18 Italian,19 Singaporean Chinese,20 and Norwegian7 populations. Furthermore, Hakonarson, et al.21 demonstrated that a study from Iceland failed to show evidence of a linkage between asthma and chromosome 7q31.2.
In contrast, Dahl, et al.22 found that ΔF508 heterozygosity was associated with an increased susceptibility to asthma in a Danish population. Additionally, studies from Greek23,24 and Spanish25 populations reported a positive association between asthma and CF heterozygosity.24 Schroeder, et al.26 suggested that obligate ΔF508 carriers are protected from asthma. However the background haplotype for ΔF508,27 which accounts for 66% of worldwide cystic fibrosis, is very rare in the Korean population.11
Besides, genetic variants at Q1352H or E217G were found to be associated with bronchiectasis and/or chronic pancreatitis in the Korean population.11 In particular, non-synonymous Q1352H and E217G mutations in the M470 background caused a 60-80% reduction in CFTR-dependent Cl- currents and HCO3- transport activities. However, we could not find any significant association at those sites in this study. In addition, Q220X and Q1291X mutations that give rise to premature stop codon can lead to aberrant function. However, there are no mutant variants in those loci in our study sample.
Several reports suggested that ΔF508 carriers have lower values of pulmonary function such as FEV1 or FVC compared to non-carriers, although no difference in the annual decline in lung function was observed between the two groups.24,28 However, Byard and Davis29 showed that there are no significant differences in spirometric values between CFTR gene mutation carriers and non-carriers. In this study, we did not have any significant correlation between spirometric values and CFTR gene mutations in the 14 mutations (Table 2, data not shown).
It is worth considering some limitations of our study. The sample size was too small and we did not investigate the full sequence of the CFTR gene. Further study is recommended to verify the results based on our pilot study.
We conclude that this study has failed to produce evidence in support of the notion that CFTR genetic variations identified in the Korean population significantly influences the expression of the asthmatic phenotype.


 XML Download
XML Download