

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The anticoagulation warfarin is a commonly prescribed medication that has a narrow therapeutic index and displays high inter- and intrasubject variability in response. In the community there is also widespread, often unreported, self-medication with a range of herbal medicines. The opportunity for potentially life-threatening interactions between herbal medications and warfarin is thus high.1 Shengmai-yin is one such herbal medicine that is commonly used for coronary heart disease, cardiogenic shock, and septic shock for promoting microcirculation and decreasing blood viscosity as well for a wide range of the other indications.2-4 However, relatively little is known about shengmai-yin drug interactions. This is the first report of an adverse interaction between warfarin and a combination herbal product, shengmai-yin, resulting in cerebral bleeding.
CASE REPORT
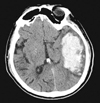
A 71-year-old man was admitted to the intensive care unit following consciousness disturbance for 5 hours. His initial Glasgow Coma Scale (GCS) score was 7. He had right hemiplegia and active pupils, 3 mm on the two sides. Head computed tomography (CT) on admission showed an intracerebral hemotoma in the left temporoparietal region causing marked midline shift to the right, and a tubular high-density area in the left temporal lobe (Fig. 1). Laboratory studies revealed prothrombin time (PT) was prolonged to 66 seconds with an international normalized ratio (INR) 5.08. Renal and liver function tests were normal. Chest X-ray revealed no abnormality.
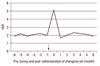
The patient received aortic valve and mitral valve replacement one year ago and his heart function restored to New York Heart Association Class I. He was receiving warfarin therapy after surgery. He was followed in the medical clinic every 4 weeks. His INR was mostly in the range of 1.8-2.2 (Fig. 2), except during the dose titration in the first month of warfarin therapy. During the medical clinical visit a half of year ago, the patient felt well and he stated that he was taking all of the prescribed drugs following medical advice. The INR value was 1.9 three month ago and 2.0 one month ago. The patient's blood pressure has been well-controlled since he was diagnosed hypertension.
When admitted to the intensive care unit (ICU), the patient's wife stated that he only took the prescribed medications. There were no recent changes in the amount of vegetable (vitamin K) intake. On further questioning, however, the old lady said that the patient started to take a kind of Chinese herb called shengmai-yin (Kanghua pharma Inc., Jiaozuo, Henan, China), because he believed that shengmai-yin was helpful for his heart disease. He took it 10 mL daily beginning 7 days prior to admission.
On admission to the ICU, vitamin K1 40 mg was administered first and the INR decreased to 1.67, PT to 19 seconds. Craniectomy was performed to remove the intracerebral hematoma under general anesthesia. He remained confused and restless for 2 days, but then showed progressive recovery in a consciousness level as well as motor and verbal functions. The patient was discharged on warfarin dose 2.25 mg daily; his INR was 2.0. Lotensin 5 mg daily continued. He was advised not to take shengmai-yin and other herbal medicines because of the risk of loss of anticoagulation control. After 6 months, he was able to walk by himself, without any bleeding complications and alterations in INR to a value > 3.0.
DISCUSSION
During the first year of warfarin therapy, this patient never had any bleeding complications and alterations in INR to a value > 5.0 until he took the Chinese herb, shengmai-yin. In the absence of other precipitating factors, the temporal relationship between shengmai-yin consumption and the onset of bleeding in the brain suggested that this herbal product was responsible for the loss of anticoagulation control. An objective causality assessment using the Drug Interaction Probability Scale (DIPS)5 revealed that the observed reaction was highly probable to be related to concomitant use of warfarin and herbal product, shengmai-yin.
Shengmai-yin is a popular Chinese combination herbal product, which was developed on the base of a thousand-year-old traditional Chinese medicine prescription, shengmai-san. Traditional Chinese theory believed that shengmai-yin has the effect of supplementing Qi and nourishing Yin, fu mai and improving peripheral circulation. Shengmai-san is commonly used for its effect on oxidative damage in heart, brain, and other tissues.6-8 Although it has been applied for heart and blood diseases, routinely and prophylactically for thousands of years in China,2-4 little available clinical data showed that it could cause apparent bleeding. It contains hongsheng (red ginseng), maidong (liriope), and wuweizi (schisandra chinensis). There are many different types of red ginseng, such as rhizoma ginseng rhbra, radix ginseng rhbra (1 year), radix ginseng rhbra (2 year), North Korea radix ginseng rhbra, radix ginseng rhbra (ordinary), and radix ginseng rhbra (xinkaihe). All contains different amounts of ginsenoside Rg1, Re, and Rb1.9 Case reports and healthy volunteer trials have had conflicting results, some reporting a potentiating10-14 and others a reductive influence.15-19 Previous studies10-13 have suggested that red ginseng was associated with an altered INR occurred in this patient. In 1998, Nakajima, et al.12 demonstrated that red ginseng was observed to increase the production of Interleukin 1 beta, which is known to play important roles in the homeostatic activities of the human body such as increasing the production of tissue plasminogen activators, which suppress the formation of thrombin in the blood coagulation and fibrinolysis mechanisms. In a later study, Lü, et al.14 confirmed these findings. Their study revealed that Rg1 down regulates plasminogen inhibitor 1 (PAI-1), tissue factor pathway inhibitor, coagulation factor XIII, A1, and, coagulation factor II (thrombin) receptor (F2R). A recent study by Jin, et al.10 suggested that Korean red ginseng has a potent antithrombotic effect in vivo, which may be due to antiplatelet rather that anticoagulation activity. In contrast, Jiang et al.15 showed that co-administration of warfarin with ginseng did not affect the pharmacokinetics or pharmacodynamics of either S-warfarin or R-warfarin in healthy subjects in 2004. Recently, Lee, et al.16 also found that co-administration of panax ginseng and warfarin in ischemic stroke patients does not influence the pharmacologic action of warfarin. Later study by Jiang, et al.17 demonstrated that Asian ginseng could actually modestly increase the clearance of warfarin and decrease its effectiveness. In addition, Mu, et al.20 found that the administration of wuweizi, another essential component of shengmai-yin, can increase the metabolism and decrease the levels of warfarin in animal models due to CYP2C9 induction.
Drug interactions occur at varying rates in patients. The causes for variability include Genetics, diseases, diet/nutrition, environment, smoking, and alcohol use. The individual Genetic traits underlying increased or decreased the effect of drug co-administered other drugs are unknown. The Genetic trait needs further investigation for this case.
Intracerebral bleeds due to trauma, rupture of an aneurysm or arteriovenous malformation (AVM), and bleeding within a tumor. A very small proportion is due to cerebral venous sinus thrombosis. High blood pressure raises the risk of spontaneous intracerebral hemorrhage by two to six times.21 The patient suffered from hypertention for many years, but he took antihypertensive (agent) at a regular base and blood pressure was well-controlled. He had no trauma history and head CT showed no other abnormalities.
However, the effect of shengmai-yin on coagulation progress was controversial. In this patient, loss of anticoagulation control was more likely after consumption of shengmai-yin, possibly due to its potentiating effect on the normal coagulation progress. Warfarin has a narrow therapeutic index. Patients should be counseled to avoid herbal medication that can interact with warfarin. It is important to take a detailed history regarding the use of all drugs and herbal medicines, especially in patients with anticoagulant therapy.
 XML Download
XML Download