

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Internal hernias are uncommon and difficult to clinically diagnose. They are defined as herniation of a viscus through an intraperitoneal orifice or aperture within the confines of the peritoneal cavity.1 Paraduodenal hernias, although rare in clinical practice, represent the most common type of congenital internal hernia.1-7 Presentation can range from acute intestinal obstruction (the most common clinical presentation) to an extended history of vague abdominal pain, often relived by changes in position.2,5,8 We present a case of a patient who underwent laparotomy for atypical symptoms due to a left paraduodenal hernia.
CASE REPORT
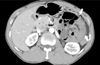
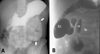
A 38-year-old man presented to the emergency department complaining of left flank pain and vomiting. He could not stay in a supine position because of flank pain. He had no remarkable medical history. Specifically, he had no history of abdominal surgery. A physical examination revealed a slightly distended abdomen and left costovertebral angle tenderness. Blood analysis, urine analysis, and a plain abdominal radiography showed no abnormalities, except for leukocytosis of 11,200 cells/mL. Abdominal ultrasonography showed mild left hydronephrosis with no ureteral obstruction. His pain was initially thought to be caused by acute pyelonephritis. Over the few hours following admission, the patient complained of increased left flank pain and vomiting. Computed tomography showed a cluster of small bowel loops encased in a sac located amidst the stomach, the pancreas, and the left kidney, the latter of which was normal without hydronephrosis (Fig. 1). The diagnosis of a left paraduodenal hernia was made using an upper gastrointestinal series with small bowel follow-through, which revealed loops of jejunum clumping over the left upper quadrant of the abdomen (Fig. 2A). These loops were identified in the posterior wall of the stomach (Fig. 2B). With the patient's left flank pain progressively worsening, a laparotomy was performed via a midline incision. Exploration revealed that about one third of the proximal small bowel was encapsulated in a peritoneal sac formed by a peritoneal flap of the left mesentery. The orifice of the hernia sac was located below the inferior mesenteric vein, with engorgement and crowding (Fig. 3). The small bowel was viable and was easily reduced after herniotomy. The defects in the left mesocolon and the hernia orifice were closed. Further inspection of the peritoneal cavity revealed no other abnormality. Postoperatively, the patient had an uneventful recovery and was discharged on postoperative day 5. During the follow-up period of 1 year, he remained completely free of symptoms.
DISCUSSION
Andrews first described the currently accepted mechanism of paraduodenal hernia formation as a type of malrotation.4 As the midgut rotates in the 5th to 11th weeks of gestation, the mesentery becomes fused to the posterior abdominal structures from the ligament of Treitz inferolaterally to the right iliac fossa. This process of attachment may be complete, except for a small zone just below the duodeno-jejunal junction where the former emerges from its retroperitoneal position. The pocket thus formed may extend to the right behind the mesentery, behind the ascending colon, or to the left behind the descending mesocolon and descending colon. When the small bowel enters these two spaces, the resulting lesions are called right or left paraduodenal hernias.1 Although paraduodenal hernias are congenital, most patients present between the 4th and 6th decades of life (mean age 38.5 years).1-3 Men are commonly 3 times more affected than women are, and left-sided paraduodenal hernias are more common than right-sided ones are, representing 75% of cases.1-8 The most common presentation is acute small bowel obstruction with a background of recurrent, vague abdominal pain. Symptoms are often postprandial, and pain may be relieved when the patient is supine.5,8 However, the present case was characterized by atypical symptoms: left flank pain with vomiting, aggravated in the supine position. Symptoms may result from retroperitoneal mass effect. Although the laboratory findings were inconclusive in this patient, his clinical picture was thought to be consistent with acute pyelonephritis. The clinical symptoms of left paraduodenal hernia formation are variable, as are the gastrointestinal manifestations, such as abdominal pain, nausea, and vomiting. The present patient represents a rare case of left paraduodenal hernia presenting with left flank pain.
The diagnosis of paraduodenal hernia formation is often difficult to make due to ambiguous presentation. This makes CT scanning a valuable initial tool for investigation.3 The most common radiologic signs of left paraduodenal hernia formation include clustering of small bowel loops, a saclike mass with encapsulation at or above the ligament of Treitz, duodenojejunal junction depression, mass effect on the posterior stomach wall, engorgement and crowding of the mesentery vessels with frequent right displacement of the main mesenteric trunk, and depression of the transverse colon.9 Barium contrast studies are most effectively performed during a symptomatic period. In contrast to follow-through studies, the small bowel is usually located to the left of the midline with a well-circumscribed edge that corresponds to the hernia sac.5,9-11 There may also be a delay in the passage of contrast through the small bowel loops with changes in the patient's position. These features were readily apparent in our patient. However, because all the above investigations may be normal, especially in chronic intermittent cases, the elective diagnosis of a paraduodenal hernia is relatively infrequent.5
Once diagnosed, left paraduodenal hernias should be surgically repaired because they carry an approximately 50% lifetime risk of incarceration, leading to bowel obstruction and strangulation.2,3,5,8 The mortality rate associated with paraduodenal hernias is not clear, but it has been stated to be 20-50%.5 Reports prior to 1981 indicate a high mortality,12 but recent improvements in radiological facilities have allowed for earlier diagnosis and elective treatment, leading to better outcomes.3,5 Surgical treatment of left paraduodenal hernias follows the basic principles of hernia surgery: reduction of the contents, restoration of normal anatomy, and repair of the defect.1-8 Recently, there have been reports of laparoscopic left paraduodenal hernia repair.8,13
In conclusion, paraduodenal hernias are an unusual cause of intestinal obstruction, but one with which all surgeons should be familiar. Because the presentation of a left paraduodenal hernia is ambiguous and variable, it is impossible to establish a correct diagnosis through physical examination alone. Early surgical intervention should be performed to minimize the morbidity and mortality associated with this condition.

 XML Download
XML Download