

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Patients with bipolar disorder have recurrent fluctuating mood episodes with functional impairment,1 which might induce chronic distress and increase suicide-related behaviors.2 The prevalence of attempted suicide and suicide completion are markedly higher in bipolar patients than in the general population.3,4 Previous studies have found that 9-60% of patients with bipolar disorder die from suicide and 15-56% of patients attempt suicide.5 In Korea, the suicide attempt rate has been reported to be 1.0% for the general population, 3.0% for college students, 6.4% for high school students, and 4.3% for middle school students.6-8 A Korean study regarding bipolar patients found that the prevalence of suicide attempts in patients with bipolar disorder was 7.5%, with this being higher for patients with bipolar II disorder (26.5%) than for those with bipolar I disorder (5%).9,10 Suicide is the most terrible consequence of bipolar disorder, and suicide-related behaviors are significant impediments to improving the treatment outcome and quality of life in bipolar disorder.
Many studies of suicide in bipolar disorder have suggested that various sociodemographic and clinical factors increase the risk of suicide attempts in bipolar disorder, such as previous suicide attempts,11 suicide idea,12,13 depressed mood,14 severe depression,13,15 comorbid illness in bipolar II disorder,16 comorbid alcohol abuse or dependence,17,18 comorbid axis II diagnosis,15 hopelessness at the admission,13 duration of illness,13,19 family history of suicide,18 having interpersonal and occupational problems,20 and early onset of illness.20,21 A recent meta-analysis revealed that previous suicide attempts and hopelessness were the main risk factors for suicide, and that early onset, depressive symptoms, and family history of suicide were the main risk factors for nonfatal suicide-related behavior.22 Clinicians should therefore pay more attention to risk factors for suicide attempts in bipolar patients in order to reduce the prevalence of suicide and suicide-related behaviors. However, the sociodemographic and clinical features related to the risk of suicide attempts remain complex, including those in Korea.
We investigated the descriptive characteristics of suicide attempts and the risk factors for suicide attempts in Korean bipolar patients by assessing sociodemographic factors, clinical factors, and the methods of suicide attempts using retrospective reviews of medical records. We thought it is quite likely that sociodemographic factors and clinical characteristics found to be associated with suicide attempt in previous studies might be associated with suicide attempt.
MATERIALS AND METHODS
Subjects
This is part of a retrospective chart review study about clinical characteristics of inpatient bipolar disorder. We reviewed medical records of all 601 patients who were admitted to the psychiatric wards in one mental hospital and three general hospitals (Yonsei University Severance Hospital, Yonsei University Severance Mental Health Hospital, Hallym University Sacred Heart Hospital, and National Health Insurance Corporation Ilsan Hospital) from January 2001 to December 2006 and diagnosed with bipolar disorder type I, II, or not otherwise specified (NOS) according to the Diagnostic and Statistical Manual 4th Edition (DSM-IV) criteria.23 This study included all admitted patients and we tried to review their inpatient medical records during this period. Cases of presence of comorbid organic mental illness, presence of severe medical illness (possibility of affect misdiagnosis of bipolar disorder), and change of major psychiatric diagnosis (e.q., from bipolar disorder to schizoaffective disorder) in consecutive admissions were excluded. This study was approved by the institutional review board of Severance Mental Health Hospital.
Review procedure
Index admission was defined as the first admission to be diagnosed as bipolar disorder during the study period. Past histories of suicide attempts were taken from medical records. Suicide attempt was defined as self-harm with the intention to die during the patient's lifetime. Only suicidal gestures were not defined as suicide attempts when medical records were clearly described as suicidal gestures. Focusing on serious suicide attempts, we defined nonattempters as the patients who have had a suicide idea or plan but did not attempt suicide and who have never had a suicide idea or plan. We defined the onset of bipolar disorder as the first time of any mood episode during the patient's lifetime. The duration of illness was defined as a period between the first mood episode and the index admission. We assessed the sociodemographic factors including age at admission, sex, education level, marital and employment status, and clinical characteristics including onset age, duration of illness, mood episode characteristics, subtype, family history of psychiatric illness, comorbidity, psychotic features and global assessment of functioning (GAF) score at admission, and methods used in suicide attempts at the index admission. Psychotic features were defined as any kind of hallucination or delusions at the index admission.
Psychiatric comorbidities were defined as any kind of psychiatric illnesses other than bipolar disorder, comprising alcohol dependence, panic disorder, obsessive compulsive disorder, eating disorder, personality disorder, and other anxiety disorders. Medical comorbidities were defined as any kind of moderate to severe physical illnesses that needed long-term treatment. We excluded the records of 22 patients due to lack of information regarding suicide history and 579 medical records of bipolar patients were included in the final analyses. Medical records were systematically reviewed by four senior psychiatric residents in three consensus meetings. We gathered these data mainly from summary records at the index admission, but we also investigated admission notes and progress notes to complement insufficient data. When the data could not be identified, we assigned these data as missing for only that item.
Statistical analyses
Bipolar patients were divided into two groups based on the history of suicide attempt. Demographic and clinical characteristics were compared between these two groups. Descriptive analyses were applied to the methods of suicide attempts and age-distribution of suicide attempters.
Because the age at index admission was significantly lower in the attempter group compared to the nonattempter group, univariate analysis of covariance were used to compare onset age, level of education, duration of illness, number of admissions, and score of Global Assessment of Functioning (GAF) between the attempter and nonattempter groups controlling for age at the index admission as a covariate. Chi-square tests were used to compare the frequencies of gender, employment status, marital status, family history of psychiatric disorder, subtype of bipolar disorder, polarity of initial mood episode, psychiatric and medical comorbidities, and accompanying psychotic features between the attempter and nonattempter groups. We applied Bonferroni correction over the univariate analysis of covariance and chi-squared tests for clinical characteristic variables and considered it significant when the two-sided probability was less than 0.0045 (0.05/11). Finally, we performed logistic regression analysis to simultaneously identify risk factors that were significantly associated with suicide attempts. Results were considered significant when the two-sided probability was less than 0.05 in the logistic regression analysis. Statistical analyses were performed using SPSS [version 12.0 for windows (SPSS Inc, Chicago, IL, USA)].
RESULTS
Demographic characteristics of the subjects
The 579 subjects who were included in the final analysis was comprised of 262 (45.3%) men and 317 (54.7%) women. Their mean education and durations of illness were 12.7 years and 6.95 years, respectively. They were comprised of 539 (93.1%) subjects with bipolar I disorder, 21 (3.6%) with bipolar II disorder, and 19 (3.3%) with bipolar disorder NOS.
Characteristics of suicide attempters
Suicide attempters were 76 (13.1%) patients among the 579 subjects. Drug overdose (26/76, 34.2%) was the most common method of suicide attempt, followed by wrist cutting (15/76, 19.7%), jumping out of a window (10/76, 13.2%), and unknown (14/76, 18.4%) and hanging (8/76, 10.5%). The combination of jumping out of a window and drug overdose (1, 1.3%), hanging with drug overdose (1, 1.3%), and self-burning (1, 1.3%) were all reported once. Suicide attempts were most frequent among those aged 20-29 years (42.9%), followed by those aged 30-39 years (25.0%), older than 40 years (23.2%), and 10-19 years (8.9%).
Comparisons of demographic and clinical data between attempter and nonattempter groups
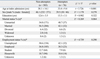
As indicated in Table 1, age at index admission was lower in the attempter group than in the nonattempter group. Other demographic data including sex distribution, level of education, employment status, and marital status did not differ between the two groups.
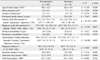
Depressive first episodes were significantly higher in the attempter group than in the nonattempter group. Onset age was not significantly different between the two groups after controlling for age at the index admission. The prevalence of mixed episodes [14.3% (2/14) vs. 2.3% (11/531)] and depressive episodes [28.5% (4/14) vs. 7.0% (11/531)] of bipolar II patients at the index admission was significantly higher than those of bipolar I patients (p < 0.001). As indicated in Table 2, there was no significant difference between the groups regarding illness duration, number of admission, proportion of family history of psychiatric disorder, diagnosis at first and index admission, psychiatric or medical comorbidity, diagnosis subtype, psychotic features, admission days, and GAF scores.
Logistic regression analysis
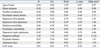
The results of the logistic regression analysis of the association between suicide attempts and candidate clinical risk factors showing significant differences between the two groups is summarized in Table 3. The history of suicide attempts was significantly associated with the polarity of initial mood episodes and diagnosis subtypes, but not with other clinical factors.
DISCUSSION
In this study, we found two significant risk factors associated with suicide attempts in Korean bipolar patients. The depressive first episode and bipolar subtype were associated with a history of suicide attempt in bipolar patients.
First, we found that the patients with depressive first episodes appear to be higher in suicide attempters. A previous study emphasized the importance of the polarity and initial mood episode as a measure of predicting the subsequent course and illness severity.23 Bipolar patients with a depressive episode at their initial admission or first episode tend to have a depressed mood at the next episode.24,25 Moreover, 60% of suicide attempters with depressive episodes commit suicide at the first mood episode.26 Prolonged exposure to depressive episodes might increase the risk of suicide attempts in bipolar patients and poor prognostic factor in suicide related behavior.27 An initial depressive episode might relate to misdiagnose it as unipolar depression and may lead to mistreatment. Two-thirds of bipolar patients are misdiagnosed as unipolar depression at first, and one-third of bipolar patients did not have the correct diagnosis until 10 years after the first treatment.28 In depressive episodes, there are no suicide protecting factors such as grandiosity and elated mood.29 Therefore, more attention should be paid to the possibility of bipolar depression among depressive patients, especially at the first treatment or episode through comprehensive screening.
Second, we could observe that bipolar II patients have a higher risk for suicide attempts.
Bipolar II patients are known to have greater risk of suicide than bipolar I patients.26,30 Bipolar II patients show a predominantly depressive mood, mood lability, and mixed nature.31,32 Bipolar II patients are likely to have depressive or mixed episodes at hospital admission rather than bipolar I patients. Bipolar II patients have more cyclothymic temperament,33 rapid cycling,34 and mixed episodes35 that may be associated with suicide risks.36 Considering these results, we could infer that depressive or mixed episodes of bipolar II patients might account for the higher suicide rate than in the bipolar I patients. In addition, bipolar II patients usually have a low insight level, do not comply with psychiatric treatment well, and have a tendency not to receive prophylactic treatment.37 Absence of prophylactic treatment and predominant major depressive episodes might dedicate suicide attempts in bipolar patients.
We found no significant differences in gender distribution, education level, employment status, marital status, and other clinical characteristics except for the initial mood episode, onset age, and diagnosis subtype between attempters and nonattempters. A recent meta-analysis found that gender, employment status, marital status, and family history of affective disorders did not increase the risk of suicide attempts in bipolar patients.22
The family history of psychiatric disorders did not differ significantly between the attempter and nonattempter groups. A previous study suggested that family history of bipolar disorder is a risk factor for suicide.18 The relation of clinical variables such as psychotic features and suicide risk were not found. We cannot conclude that there are no relations between psychotic features and suicide attempt due to the insufficient notes regarding the psychotic features at the time of the suicide attempt. We could not perform a definitive psychiatric diagnosis of bipolar family members due to this study design.
This study has some limitations to be considered. First, data of this study were derived from patients of multiple centers to include enough subjects to find risk factors of suicide attempt in Korean bipolar patients. The heterogeneity of the data could be problematic, but there was no significant difference in demographic characteristics including age, gender, education level, and clinical characteristics including suicide history, age of onset, and duration of illness between four hospitals. Second, this study has a retrospective design by reviewing medical records. Further interviews for clarifying ambiguous data was not possible for discriminating the presence of family psychiatric history and comorbidity of patients. Underreporting or underdetection of suicide-related behavior of the patients in this study cannot be excluded. However, patients were diagnosed by at least three doctors, junior and senior residents, and a professor, which makes the data more reliable. And for having a consensus in the diagnosis among doctors, we had weekly meetings for the diagnosis in these hospitals. Fourth, there are possibilities of including suicidal gestures. We tried to exclude cases of suicidal gestures by checking the intention to die in the medical records, but we cannot exclude the possibility completely. Finally, the possibility of selecting patients with severe psychopathology may also exist because all participating hospitals are university hospitals which are at the end point of the Korean medical system.
Psychological trauma early in life is known to be associated with self-harming in general,38 but this issue also could not be considered due to a lack of data. Prospective studies addressing more comprehensive candidate risk factors for suicide and suicide attempts in bipolar disorder are necessary in Korea.
Suicide is a major concern and health issue in bipolar disorder. A regular and continuous monitoring schedule for the risk of suicide and suicide-related behaviors should be included in the comprehensive management of bipolar disorder. In particular, careful evaluation and effective management of bipolar depression among patients with mood disorder during major depressive episodes is necessary to prevent suicide attempts in bipolar disorder.
 XML Download
XML Download