

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
During the development of the brain cortex, a radial glial fiber system forms and primitive neurons migrate from the ependymal surface to the cortex in a 1-to-1 matching pattern. If the migration process is interrupted, heterotopic gray matter forms along the route of neuronal migration and can take an island-shaped nodular form or an aggregated band form.1,2 Heterotopia is often a cause of intractable seizures and psychiatric disorders,3-5 but it can sometimes be detected in asymptomatic patients. When it is localized in form and found to be an epileptogenic lesion, surgical resection is the treatment of choice, and precise localization is essential.
Diffusion tensor imaging (DTI) is a recently introduced MR technique that can show white matter integrity and the direction of fiber arrangement in vivo. Its clinical application is now increasing in frequency. White matter bundles have higher anisotropy than gray matter because of the arrangement of fibers and increased water diffusion along a specific axis. Heterotopic gray matter, the neurons arrested during migration, is likely to have significant anisotropy due to its developmental background.6
The purpose of this study was to assess the utility of DTI in the evaluation of heterotopia and to improve understanding of the pathophysiologic mechanism of anomalous neuronal migration.
MATERIALS AND METHODS
Diffusion-weighted imaging data from 11 patients (M : F = 7 : 4, aged from 1 to 22 years, mean = 12.3 years) who visited the epilepsy clinic and received a routine seizure protocol MRI exam and FDG-PET images were retrospectively analyzed. The exam included anatomical T2 weighted axial, FLAIR axial, oblique T2 weighted coronal, 3-D gradient echo T1 weighted coronal, and diffusion tensor imaging. MRI was performed using a 1.5T or 3.0T scanner (Achieva, Philips Medical Systems, Best, Netherlands) with an 8-channel Sensitivity Encoding (SENSE) head coil. DTI was performed using single-shot spin echo-echo planar imaging with SENSE factor 2. The imaging parameters were as follows: 220-mm field of view (FOV), 2 mm iso-voxel data acquisition with 2-mm slice thickness, TE = short as low as 48 ms at 3.0T and 70 ms at 1.5T scanner; TR = 6,599-8,280-ms according to slice number; number of signal acquisition = 2, b = 600 s/mm2, and 32-different diffusion gradient directions. The data were processed on a PC equipped with the Philips research imaging development environment (PRIDE) research software package (Philips Medical Systems, Best, Netherlands) or operating console of MR scanner. Semi-quantitative analysis was performed for regions of interest (ROI) settled on heterotopic gray matter (HGM), and fractional anisotropy (FA) was measured. The FA of deep gray matter (DGM) from thalamus and cortical gray matter (CGM) were also measured. Cortical gray matter for the contralateral normal control was selected from slices showing heterotopic gray matter. Statistical analysis of DGM, HGM, and CGM was performed using ANOVA.
RESULTS
Four patients had classical band heterotopia, i.e., a double-cortex with a linear gray-matter signal band in the white matter and intervening white matter between the heterotopia and normal cortex. Seven patients showed nodular heterotopia, including associated dysplastic cortex, and four of these had agenesis of the corpus callosum. For anatomical T2 weighted, FLAIR and 3-D gradient echo T1 weighted MRI, heterotopic gray matter showed the same signal intensity as the normal cortex. On FA maps, HGM showed higher signal intensity than that of the cerebral cortex or deep gray matter. Band-like high signal areas were noted on FA maps in the cases of band heterotopia (Fig. 1). All HGM showed a higher signal than that of CGM and a lower signal than those of DGM and normal white matter. On FDG-PET scan, heterotopic gray matter showed similar activity as cortical or deep gray matter, suggesting of high glucose metabolism as normal gray matter (Fig. 1).
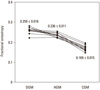
On quantitative analysis, the FA of heterotopic gray matter was higher than that of cortical gray matter (0.236 ± 0.011 vs. 0.169 ± 0.015, p < 0.01, one way ANOVA), and slightly lower than that of deep gray matter (0.236 ± 0.011 vs. 0.259 ± 0.016, p < 0.01) (Fig. 2).
DISCUSSION
Heterotopia is a type of cortical malformation in which the normal radial migration of neurons is arrested, causing gray matter tissue to be embedded in the white matter.2 The etiology of heterotopia is unclear; some genetic factors have been reported,4,7 while sporadic cases have also been described.8 Prenatal infection is also known to be a factor causing the arrest of neuronal migration, resulting in the formation of heterotopic gray matter between the ependyma and cortex. Heterotopia has been divided into three groups based on clinical and imaging characteristics: subependymal, subcortical, and band heterotopia. On conventional MR imaging, heterotopic gray matter has signal intensity similar to that of normal gray matter and can appear nodular or curvilinear.9 Functional MRI has revealed an activating signal at the heterotopic cortex,10-12 and MR spectroscopy has shown efficacy in differentiating heterotopia from low-grade tumors.13 Heterotopic neurons are considered mature since their metabolites are same as those of normal cortex.
Heterotopia has a wide range of clinical manifestations from asymptomatic to generalized tonic seizures.5 A precise evaluation before surgery is critical because heterotopic gray matter is epileptogenic and can also affect major motor, vision, or sensory functions. MRI is the basic tool used to accomplish this.
During brain development, neurons migrate from the ependymal surface to the cortex along the cytoarchitectural skeleton. Arrest during migration is the key pathology of heterotopia. Eriksson, et al.6 reported increased fractional anisotropy of band heterotopia on DTI. They hypothesized that high anisotropy of ectopic gray matter was due to the nature of neuronal growth and partial volume averaging of the surrounding white matter. Previous histopathological study revealed that heterotopia consisted of unlayered small or medium sized rounded or pyramidal neurons, occasionally interrupted by small bundles of fibers.14 Another study hypothesized that increased directivity of HGM indicated that the tissue was in the process of directional migration during neurodevelopment.15
In conclusion, this study suggests that increased anisotropy of heterotopic gray matter results from its histological nature and embryogenetic mechanism, i.e., gray matter tissue in white matter bundles and a radial growth pattern of neuronal migration. The results of this study will provide a better understanding of neuronal migration and the pathogenesis of ectopic gray matter during neurodevelopement.

 XML Download
XML Download