

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The prevalence of type 2 diabetes has been rapidly rising worldwide. In Korea, the prevalence of diabetes (95% of which were cases of type 2 diabetes) has increased from 1% of the general population in the 1970s to 13.5% of men and 10.7% of women aged 30 years or more in 2000.1 Chronic kidney disease (CKD) is one of the major complications of type 2 diabetes, and is the leading cause of endstage renal disease (ESRD), accounting for approximately 40% of new cases of ESRD every year.2 Early detection and treatment of CKD in patients with type 2 diabetes can prevent or retard the progression to ESRD.
Several studies have reported positive associations between inflammatory biomarkers and ESRD3-5 or advanced kidney failure.6 However, few studies have provided information on the relation between inflammation and mild to moderate CKD. And to the best of our knowledge, only two studies have been performed in patients with type 2 diabetes7,8 and no study has been performed in Asian patients with type 2 diabetes. Type 2 diabetes is considered a chronic inflammatory condition resulting from obesity-induced dysregulation of adipocytes, which produce excessive inflammatory cytokines such as tumor necrosis factor (TNF-α), interleukin-6 (IL-6), and C-reactive protein (CRP).9 This persistent inflammatory state further contributes to insulin resistance10 and abnormal endothelial vascular reactivity.11 Chronic inflammation exacerbates kidney damage through mechanisms of vascular endothelial cell impairments. On the other hand, adiponectin, secreted by adipose tissue, is considered to be an important modulator of insulin sensitivity and its concentration is reduced in patients with type 2 diabetes and CKD, suggesting its various protective functions as an anti-diabetic and anti-inflammatory factor.8,12 Previous studies, however, did not include both inflammatory and anti-inflammatory biomarkers. In addition, no attempt to assess dietary intake, which is an important risk factor for both type 2 diabetes and CKD,2,13 was made in the aforementioned studies.
Therefore, the objective of the present study was to examine the relation between the risk of CKD and inflammatory (TNF-α, IL-6, and CRP) and anti-inflammatory (adiponectin) biomarkers in patients with type 2 diabetes. Our hypothesis was that an inflammatory biomarker would be positively associated and an anti-inflammatory biomarker negatively associated with the risk of CKD in patients with type 2 diabetes.
MATERIALS AND METHODS
Study subjects
All participants were patients with type 2 diabetes who visited one of two diabetes clinics in Seoul, Korea. For an ongoing, prospective study of patients with type 2 diabetes, 847 subjects (439 men and 408 women, aged 40-85 years), without coronary heart disease or cerebrovascular disease, were randomly selected and interviewed for a baseline investigation from September 2005 to September 2007. In the baseline sample, 196 subjects were excluded because no data were available on their plasma creatinine (n = 131), body mass index (BMI) (n = 3), or dietary intake (n = 62). Among the remaining 651 subjects, 27 were excluded due to insufficient information on their blood parameters, and a further 81 were excluded as a result of fasting blood glucose < 126 mg/dL or hemoglobin A1C (HbA1C) < 6.5%. Therefore, a total of 543 Korean patients with type 2 diabetes (284 men and 259 women; aged 40-85 years) were ultimately eligible for this analysis. Written informed consent to participate was obtained from each individual. The study protocol was approved by the Institutional Review Board of Yonsei University.
General characteristics, anthropometric measurements, and blood pressure
All subjects were individually interviewed to obtain information about general characteristics such as age as well as life-style behaviors such as smoking (non-, ex-, or current-) and regular exercise (yes/no). The duration of diagnosed type 2 diabetes, calculated by subtracting the year of diagnosis from the year of baseline survey, was obtained from a review of the medical record or was self-reported with the help of an attending endocrinologist. For anthropometric measurements, height was measured with a standiometer (Seca Inc., Hamburg, Germany) attached to a wall, weight was assessed using Inbody 4.0 (Biospace Co., Seoul, Korea), and BMI (kg/m2) was calculated. Waist circumference was measured with a tapeline (Tanita, Seoul, Korea). Systolic and diastolic blood pressures were measured after the patients had rested for 10 min in a sitting position, using an automatic blood pressure monitor (Biospace Co., Seoul, Korea), and were read by the attending endocrinologists. Hypertension was defined as a systolic blood pressure (SBP) > 140 mmHG, a diastolic blood pressure (DBP) > 90 mmHG, or as taking hypertension medication.
Dietary intake
Graduate students trained in nutrition individually interviewed each subject to assess their food consumption for the past year, using a food frequency questionnaire, which included 114 food items and had been previously validated.14 The food intake data were analyzed using Can-Pro 3.0 software (Korean Nutrition Society, Seoul, Korea) to determine nutrient intakes for energy, fat, zinc, vitamin A, vitamin C, vitamin E, and folate, and were compared to the Dietary Reference Intakes for Koreans.15
Biochemical analysis
Blood samples were taken after a minimum 12-hour overnight fast, collected in EDTA-containing tubes, and centrifuged at 3,000 rpm for 20 minutes at 4℃ (Hanil Science Industrial Co., Ltd, Seoul, Korea). The plasma samples were stored at -80℃ until analysis. Fasting serum levels of glucose, cholesterol, triglyceride, high-density lipoprotein (HDL)-cholesterol, albumin, creatinine, and blood urea nitrogen (BUN) were measured using an autoanalyzer (Cobas Mira Roche Autoanalyzer, Hoffmann-La Roche Ltd., Basel, Switzerland). Low-density lipoprotein (LDL)-cholesterol and the atherogenic index (AI) were calculated by employing the following equations described by Friedewald16 and Lauer17: LDL-cholesterol = Total cholesterol - HDL-cholesterol-(Triglyceride/5) and AI = (Total cholesterol - HDL-cholesterol)/HDL-cholesterol, respectively. HbA1C was measured by an HLC-723 G7 analyzer (Toche, Japan). Serum IL-6, TNF-α, and adiponectin concentrations were determined using enzyme linked immunosorbent assay kits (Quantikine, R & D Systems Inc., Minneapolis, MN, USA) according to the manufacturer's instructions, and were read by an ELISA reader (Spectra Max 340, Molecular Devices, Sunnyvale, CA, USA). The measurement of malonialdehyde, a biomarker of antioxidant status, was performed using a Lipid Peroxidation Assay kit (Oxford Biomedical Research, Oxford, MI, USA) according to the manufacturer's instructions.
Assessment of renal function
The estimation of glomerular filteration rate (GFR) using serum creatinine concentrations is utilized as an index of kidney function and is examined in patients with type 2 diabetes to assess for CKD. In the present study, renal function was estimated by the simplified Modification of Diet in Renal Disease equation, where GFR (mL/min per 1.73 m2) = 186.3×[(serum creatinine, mg/dL)-1.154×(age)-0.203]×0.742 (if female). The subjects were classified into a normal kidney function group (GFR ≥ 60 mL/min per 1.73 m2) and a CKD group (GFR < 60 mL/min per 1.73 m2).18
Statistical analysis
The data were expressed as means with standard errors (adjusted for age and sex) or numbers and percentages. Variables with skewed distributions were log-transformed before analysis and back-transformed for presenting within tables. The differences between subjects with and without CKD were evaluated using an analysis of covariance (ANCOVA) test after adjustments for age and sex, or a χ2 test, as appropriate. To investigate the correlations between blood glucose indicators and inflammatory markers, a partial correlation analysis controlling for age and sex was performed. Multivariable-adjusted logistic analysis was conducted to examine the odds ratio (OR) for CKD across levels of inflammatory biomarkers continuously as well as across quartiles of them. The first model was adjusted for age and sex. The second model was additionally adjusted for the duration of diagnosed type 2 diabetes, smoking, regular exercise, hypertension, fasting blood sugar, and zinc intake. All analyses were performed using SPSS version 12.0 software (SPSS Inc., Chicago, IL, USA). Statistical significance was defined as p < 0.05.
RESULTS
The general characteristics and nutrient intakes of the 543 subjects with type 2 diabetes are presented in Table 1. Of these 543 patients, 488 (89.8%) were considered to have normal kidney function and 55 (10.2%) had CKD. It was found that the type 2 diabetes patients with CKD were more likely to be female (p = 0.021), were older (p < 0.001), had a longer duration of type 2 diabetes (p = 0.008), and were more likely to have zinc intakes less than the estimated average requirement (p = 0.025).
For clinical characteristics, levels of GFR were lower (p < 0.001) and levels of creatinine (p < 0.001) and BUN (p < 0.001) higher in the subjects with CKD compared to those with normal kidney function (Table 2). Mean concentrations of fasting blood sugar were also greater in the patients with CKD (p = 0.014). In addition, the subjects with CKD had greater levels of inflammatory biomarkers such as CRP (p = 0.013) and TNF-α (p < 0.001), as expected, but they also had higher levels of the anti-inflammatory biomarker adiponectin (p = 0.008) than the normal subjects, contrary to our expectation. No differences were found in serum albumin, HbA1C, blood lipid levels, and IL-6 between the two groups.
Elevated blood glucose levels in patients with type 2 diabetes can affect concentrations of inflammatory biomarkers. Partial correlation analysis revealed a significantly positive correlation between blood glucose indicators and inflammatory biomarkers (Table 3). CRP, TNF-α, and IL-6 were significantly positively correlated with fasting blood sugar and HbA1C. Such a correlation did not exist for adiponectin.
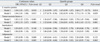
The overall results relating plasma levels of inflammatory biomarkers to the risk of CKD are shown in Table 4. The OR for CKD was positively associated with continuous values of CRP (OR = 1.04, 95% CI = 1.01-1.07; p = 0.010) and TNF-α (OR = 1.82, 95% CI = 1.32-2.53; p < 0.001) after adjustments for age and sex. The association did not change after further adjustments for duration of type 2 diabetes, smoking, exercise, hypertension, fasting blood sugar, and zinc intake. For quartiles of these biomarkers, a positive association existed between CKD risk and CRP (OR = 3.68, 95% CI = 1.77-10.75; p = 0.014) and TNF-α (OR = 3.78, 95% CI = 1.45-9.84; p = 0.002) across the lowest to highest quartiles. Furthermore, these trends did not change after adjusting other confounders (OR = 3.73, 95% CI = 1.19-11.70; p = 0.029 for CRP and OR = 4.45, 95% CI = 1.63-12.11; p = 0.001 for TNF-α). The OR for CKD tended to slightly increase with continuous values of adiponetin (OR = 1.06, 95% CI = 1.01-1.11; p = 0.005), but this trend disappeared when the values were treated as quartiles.
DISCUSSION
From our data we found a strong and graded association between CRP and TNF-α and the risk of CKD in Korean patients with type 2 diabetes. Plasma concentrations of CRP and TNF-α were significantly higher in subjects with CKD compared to those without CKD, and the risk of CKD was > 3-fold greater from the lowest to highest quartiles of CRP and TNF-α, respectively. This association appeared to be independent of other well-known putative risk factors for CKD such as age, sex, duration of diagnosed type 2 diabetes, smoking, exercise, having hypertension, fasting blood sugar concentrations, and zinc intake, based on multivariable-adjusted logistic analysis. Our results suggest that high concentrations of CRP and TNF-α may be an independent risk factor for CKD in Korean patients with type 2 diabetes.
Our findings are consistent with previously reported results. In cross-sectional analyses from the Health Professionals' Follow-Up Study of U.S. male patients with type 2 diabetes aged 40-75 years, soluble tumor necrosis factor receptor type 2 was positively associated with the risk of CKD (GFR < 60 mL/min per 1.73 m2).7 In a cross-sectional study of 23 dialyzed and 16 non-dialyzed chronic renal failure patients and 28 healthy controls in England, concentrations of CRP and TNF-α were elevated in patients with chronic renal failure as compared to the controls.19 Also shown in a previous study,8 serum adiponectin concentrations were greater in patients with CKD than in patients with normal kidney function.
Nonetheless, some studies have shown incompatible results. Among the U.S. male patients with type 2 diabetes from the Health Professionals' Follow-Up Study, no relation existed between CRP levels and CKD risk (GFR < 60 mL/min per 1.73 m2).7 Prior studies have reported a positive correlation between serum adiponectin levels and kidney function.20 Also, from another sub-study of the Health Professionals' Follow-Up Study,8 serum adiponectin concentration was negatively associated with the risk of CKD (GFR < 60 mL/min per 1.73 m2); this is unlike our results in which adiponectin was not associated with CKD risk although patients with CKD had higher mean adiponectin levels than those without. Some studies have reported elevated levels of IL-6 in patients with chronic renal failure9 or in type 2 diabetes patients with nephropathy,21 but such a difference was not found in our study. In addition, unlike findings from other studies showing a positive relation between serum lipids and the risk of CKD,7 blood lipid levels were not different between patients with CKD and those without CKD in our study.
These inconsistent results may be attributable to differences in the ethnic origins of the study populations. In this regard, ethnic-specific differences in risk factors of CKD should be considered. For example, none of the studies mentioned above, except for our current study, included dietary intake as a confounding factor for analysis. An intervention study has suggested the beneficial effects of vitamin C, vitamin E, and zinc on kidney function,22 which is similar to our results where a greater proportion of the subjects with CKD had inadequate zinc intakes. Another possible reason for the incompatible results is the use of different criteria for CKD. Therefore, a direct comparison is not possible due to the many differences in the study conditions.
Several mechanisms for the effects of CRP and TNF-α on the risk of CKD have been proposed, although the mechanisms leading to the development and progression of renal injury in type 2 diabetes are not fully understood. CRP, produced by the liver tissue, and TNF-α, synthesized primarily by monocytes and macrophages, are cytokines and sensitive indicators of inflammation. It is now evident that activated innate immunity and inflammation are related to the pathogenesis of diabetes.21 Furthermore, elevated levels of these inflammatory markers in patients with type 2 diabetes, who have chronic low-grade inflammation, play a critical role in the development of microvascular diabetic complications, including CKD, by potentiating endotherial dysfunction. Epidemiologic studies13,23 have reported that in type 2 diabetes patients with CKD who had high blood glucose levels for a prolonged period of time, poor glycemic control was markedly associated with a rapid decline in GFR and increased pro-inflammatory cytokines. Endothelial dysfunction causes increases in pro-inflammatory cytokines and anti-inflammatory cytokines.8
Consistent with our results, a positive correlation between measures of insulin resistance and plasma concentrations of CRP24 and TNF-α21 was previously reported in patients with CKD. Fasting blood sugar levels were also greater in subjects with CKD than in those without (Table 2). Overall, our data suggest that elevated blood glucose may contribute to increases in plasma concentrations of CRP and TNF-α, and tight blood glucose control is a top priority for patients with type 2 diabetes to prevent and retard the progression of diabetic complications.
Our study had several limitations that should be addressed in future studies. For example, it specifically focused on a representative group of Korean patients with type 2 diabetes. Therefore, these results cannot easily be generalized to other populations or ethnic groups. We observed an association between plasma concentrations of CRP and TNF-α and the risk of CKD in a cross-sectional setting. Therefore, it was not possible to determine whether plasma concentrations of CRP and TNF-α are a cause or consequence of CKD. The causality between serum levels of CRP and TNF-α and the risk of CKD should be evaluated in a follow-up study of the Korean population. In addition, since the levels of CRP and TNF-α increased in other cardiac conditions complicating type 2 diabetes and subsequent microvascular changes, additional biomarkers should be employed to clarify their specific direction of association to CKD. Furthermore, recall bias may have affected the subjects' self-reporting of the duration of diagnosed type 2 diabetes, although the use of a standard protocol and well-trained interviewers minimized any bias. This study also had several advantages. To date, no investigation has examined the association between inflammatory markers and CKD in Asian patients with type 2 diabetes, who have greater risk of CKD, and must be targeted for its prevention in order to further inhibit the prolonged development of type 2 diabetes complications such as ESRD and cardiovascular disease. This study also showed that elevated levels of CRP and TNF-α in patients with type 2 diabetes had significant effects on the risk of CKD after adjustments for putative risk factors for CKD including dietary intake, which is important but had not been previously investigated.
In conclusion, our results suggest that high concentrations of CRP and TNF-α may be independent risk factors for CKD in Korean patients with type 2 diabetes. Large-scale intervention studies are needed to evaluate whether lowering blood concentrations of CRP and TNF-α reduces the risk of CKD, and potential benefits of modulating CRP or TNF-α activity as therapeutic targets appear to exist in patients with type 2 diabetes.



 XML Download
XML Download