

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Anterior cervical plate application has become widely used for anterior cervical fusion. Although an anterior plate fixation addition makes the construct strong enough to avoid graft displacement and pseudoarthrosis, failure can occur from screw breakage or loosening. Screw loosening may occur following repeated removal and replacement in revision surgery or correction of a false trajectory. Polymethyl methacrylate (PMMA) augmentation has frequently been used to augment the bone screw interface, increasing pullout strength.1 However, in the field of vertebroplasty, several complications of PMMA augmentation, such as cement leakage, pulmonary embolism, high exothermic temperature (40-100℃), chemical toxicity, tissue reaction, and non-biodegradability have been reported.2,3 Many reports have been published regarding cement leakage into paraspinal, intraspinal, and venous areas.2,4,5 However, there has been no report of accidental spinal cord PMMA injection. Here, we describe the complication of injecting PMMA into the cervical spinal cord during PMMA augmentation of a damaged pilot hole.
CASE REPORT
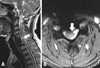
A 47-year-old male presented following a car accident. He was confused and had a forehead abrasion. Motor and sensory functions were normal. A brain computerized tomographic (CT) scan revealed no hematoma or cerebral edema. Cervical X-rays showed cervical instability at the level of C6-7. The patient was admitted for close observation with a neck collar. Two weeks later, he was alert and complained of severe posterior neck pain (VAS > 9) with bilateral upper extremity numbness. Although motor and sensory functions were intact, horizontal translation exceeded 4.0 mm, and pain was severe. Therefore, surgical stabilization was performed. As there was no facet interlocking, anterior cervical fusion was planned. After a discectomy and iliac bone graft, an anterior cervical plate (MAXIMA, U&I, Uijeongbu, South Korea) was positioned and pilot holes were tapped. However, the upper left pilot hole was stripped secondary to repeated drilling and tapping for a false trajectory correction. Although it was an unconventional method that has not been previously described, PMMA (EXOLENT SPINE, Elmdown, London, England) augmentation was performed to the damaged pilot hole. PMMA was mixed and a10 cc syringe was filled with the mixture. A sharp 16-G needle was inserted into the C6 vertebra, and PMMA was injected. Unfortunately, C-arm fluoroscope was not used during the injection procedure. The cervical plate and screws were inserted, and a portable cervical X-ray was obtained. The X-ray showed a mass lesion at the spinal canal (Fig. 1). Solumedrol was immediately injected according the NASCIS III protocol, and C6 corpectomy was promptly performed with cool saline irrigation. There was a tiny puncture point on the ventral dura. A small mass was removed through a small dural incision, centered on the puncture point (Fig. 2, left). Pial incision was extended and another small mass was removed (Fig. 2, right). A cervical X-ray showed no remnant mass lesion. Anterior reconstruction with an anterior cervical plate and mesh cage from C5 through C7 was done. Postoperatively, the patient showed Grade 3/5 left side weakness. He had Grade 1/5 impairment of the left 4th and 5th digit extension. The patient improved spontaneously (Grade 4/5) except for 4th and 5th digit extension. MR images at 6 months postoperatively showed high signal intensity at the level of C6 (Fig. 3).
DISCUSSION
Anterior cervical plate use is common with anterior cervical discectomy and fusion.6,7 Construct rigidity with anterior cervical plating is influenced by many factors, including bone to screw interface, plate to screw interface, screw triangulation, and implant design and materials.6,7 Bone to screw interface tightness is determined by insertion torque, bone mineral density, screw diameter, and screw insertion depth.6,7 However, all these factors are variable. Screw loosening frequently occurs intraoperatively from forceful insertion torque, repeated drilling or tapping of a pilot hole, and low bone mineral density.8 Fortunately, there are several salvaging methods. These include the use of thicker screws to improve holding strength,6 the use of a cemented rescue screw with bone cement injected into the hollow shaft to increase insertional torque and pullout force,9,10 and the use of an expansive screw that can be stretched after insertion, which is currently only available for posterior cervical pedicle screw fixation but not anterior plate fixation.8 PMMA has frequently been used for the fixation of various prostheses, including the spinal column.9,10 However, Pitzen, et al.11 reported that thicker screw insertion into a damaged pilot hole of the cervical vertebral body does not strengthen the screw bone interface compared with the initial strength conferred by a standard screw. In addition, the cemented rescue screw and expansive screw are not commonly available. Therefore, among the possible rescue methods, PMMA augmentation is the simplest and most effective to strengthen bone to screw interface.1,12 Reinforcement with PMMA is increasingly used in severely osteoporotic bone as well as for reinsertion after screws have been stripped by overtightening.1,12 Hernigou and Ma13 reported that PMMA bolus into the screw hole prior to insertion increased pullout strength by approximately 5%. The use of PMMA in these situations, however, may be dangerous because cement application and the amount are uncontrolled.2 Furthermore, there is a risk that PMMA may leak into the spinal canal. An additional problem is that cement heating may occur.2,3 Although mostly non-neurologic and transitory, cement can leak into the epidural, foraminal, intradiscal, paravertebral, and venous areas.2
The present case demonstrates that PMMA can be injected into the cervical spinal cord during damaged pilot hole injection. This complication was derived from two factors. The first is the use of a sharp needle, which was able to penetrate the posterior vertebral body cortex. The second was the lack of C-arm guidance. Despite the significant amount of PMMA injected, the patient recovered well. The bone cement used is known to have a lower setting temperature (minimum 62℃). This use of low exothermic cement and immediate surgical removal likely prevented more serious spinal cord damage.


 XML Download
XML Download