

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute anterior dislocation of the shoulder is reported to be commonly prevalent in athletes, and its treatment method and protocol are still debated. For early conservative management of its instability, duration and posture of fixation and method of physical therapy are not clearly defined. Conventionally, the shoulder is fixed in an internally rotated position for 3 to 6 weeks. However, recently, there have been reports to fix the externally rotated position to limit recurrence.1 There have been reports of various results in the conservative management of acute anterior dislocation of the shoulder.2-6 The authors thought that other than the generally known Bankart lesion, these lesions lead to various outcomes. Therefore, the authors studied young and active patients with anterior dislocation of the shoulder for the first time to investigate and analyze anteroinferior labrum injury types, including accompanying lesions in acute anterior dislocation of the shoulder using magnetic resonance angiography (MRA) and arthroscopy.
MATERIALS AND METHODS
Study subject
From April 2004 to April 2008, 40 patients with acute anterior dislocation of the shoulder were tested with MRA, and 36 cases (90%) with abnormal MRA findings were selected for diagnostic and surgical arthroscopy within 1 month of trauma. Their injury types of anteroinferior labrum and accompanying lesions were investigated anterogradely. Selection was based on patients having no previous history of the shoulder anterior dislocation and patients being under 30 years old. After the trauma, the dislocation had to be confirmed by an initial X-ray. If there was evidence of multidirectional instability at the ipsilateral and contralateral side, these patients were excluded from the study. If there were more than a 25% glenoidal defect, these patients were not selected for the study, either. The young age group comprised of individuals who had shown to be active previously, was chosen and the average age was 23.8 ± 4.2 years old (range: 16-30 year old). Male subjects presented in 37 cases (92.5%) and females in 3 cases (7.5%). In 24 cases (60.0%), the dominant shoulder was affected, and 16 cases (40.0%) were affected in the non-dominant side of the shoulder. Among the subjects, 28 were armed servicemen (70.0%), 8 athletes (20.0%), 2 manual laborers (5.0%), and 2 housewives (5.0%). The average duration from dislocation to surgery was 14 ± 11.3 days (range: 2-30 days). No previous history of other shoulder symptoms or instability before the dislocation was found in any patients. In all 40 cases, patients remem-bered the activities while they injured their shoulders. Sports related injuries accounted for 26 cases (65%), followed by 9 falling accidents (22.5%), and 5 traffic related accidents (12.5%). This study was approved by our institute's ethical review board and informed consent was obtained from all patients.
Surgical method & physical therapy
Arthroscopic surgery was performed by a shoulder specialist (K.D.S.), 2 residents, and a professional nurse. Patients were placed in a lateral decubitus position by leaning their trunks back posteriorly at 30 degrees, and arms flexed for 20 degrees and abducted at 45 degrees. Traction of 3 to 4 kg in weight was used. Initially, the arthroscope was placed through the posterior portal, and the anterosuperior and anteroinferior portal were created when necessary.
Suretac (Acufex, Mansfield, MA, USA) and Knotless anchor (Mitek, Westwoood, MA, USA) were used to suture labral lesions. Separated labrum was accordingly placed in order to be restored to its original anatomical location. If both superior labrum anterior-posterior lesion (SLAP) and anteroinferior labrum lesions were present, then a SLAP lesion was sutured first. Among the rotator cuff tears, for those less than a 25% partial articular side tear, debridement was performed. Complete tears were sutured using arthroscopic modified double row repair with suture-bridge technique. The fracture of the great tuberosity of humerus was reduced under arthroscopy. The fracture was fixed using cannulated screws and modified with double-row repair with suture-bridge technique.
After the surgery, abduction orthosis was worn by patients. Isometric and passive anterior flexion exercises were started on the postoperative day 1, Patients started progressive extension exercise 2 weeks after surgery. At week 3, assisted active exercises were initiated, and at week 4, the orthosis was removed to begin full range motion exercises of the joint. Therabands and dumbbells were used to strengthen the muscle six weeks after the surgery. Resistant muscle reinforcing exercises were initiated at week 12. The return to regular sports activity started 6 months after the surgery.
Evaluation method
The operator did not recommend surgery to those without an abnormal MRA finding and recorded MRA readings only. Those with abnormal MRA findings were recommended for surgery. Before performing the surgeries, the operator fully studied and recognized the readings of the MRA for those patients. A radiologist who specializes in the musculoskeletal system provided readings of the MRA results. Arthroscopic findings were unknown to the radiologist during the reading. To investigate the connection between preoperative MRA and postoperative arthroscopic diagnosis, accuracy and sensitivity to find lesions such as labrum lesions and SLAP lesions were calculated using intraoperative arthroscopic findings as a standard.
The instability of the shoulder was evaluated under general anesthesia. Grade 1 is designated to those whose humeral head was incompletely dislocated from the glenoid rim. If there is dislocation from the glenoid rim but the dislocation can be reduced spontaneously, then it is defined as grade 2. If the dislocation cannot be reduced spontaneously, then it is considered as grade 3.7,8
Impressions under the arthroscope were classified and described in 5 categories: anteroinferior labrum lesion, capsular lesion, SLAP lesion, bony structure, and rotator cuff lesions. Abnormal anteroinferior labral lesions were classified into the Perthes lesion, Bankart lesion, anterior labrum periosteal sleeve avulsion lesion (ALPSA) lesion, bony Bankart lesion, and glenoid articular rim disruption (GLAD) lesions. Among them, the ALPSA lesion was separated into two subgroups, free ALPSA lesion and adherent ALPSA lesion. The distinction was based on whether this eventrated ALPSA lesion was in the inferior-inner side of the anterior glenoid rim or the adherent.
Through the posterior portal, a calibrated arthroscopic probe was used to measure and quantify the degree of anterior glenoid bone loss if any, with reference to the central bare spot of glenoid.
An instability test (apprehension sign and relocation test) was performed by 2 orthopaedic specialists in the outpatient clinic. For the apprehension test, a patient was positioned in the supine position, his shoulder was abducted and externally rotated for 90 degrees until the patient felt discomfort. The relocation test observed whether a patient no longer feels anxiety when pressure was applied from the posterior to the proximal anterior of the upper limb.
During the follow-up, Rowe's and Zarins' evaluation methods9 were used to analyze shoulder function. It consists of four subscales: 1) function, 2) pain, 3) stability, and 4) range of motion of shoulder. For each standard, a score of 50 was given to function, 10 for existence of pain, 30 for stability, and 10 for range of motion. A score of over 90 was classified as excellent, between 70 and 89 good, 40 to 69 fair, and less than 39 poor.
RESULTS
Of those 40 with acute anterior dislocation of the shoulder tested with MRA, 4 patients (10%) did not show any abnormalities and did not undergo arthroscopic treatment. For those 36 patients (90%) who underwent arthroscopic treatment, instability was tested under general anesthesia. 6 cases (16.6%) were found to be grade 1. Grade 2 included 15 cases (41.6%), and 15 cases (41.6%) were classified as grade 3. Hemarthrosis was observed in 34 cases (94.4%). More than 25% of glenoidal defect and drive through sign were not discovered in any case.
Accompanying lesion
Anteroinferior labrum lesion was observed in 25 cases (62.5%). Among those 25 cases, Perthes lesion was found in 3 cases (12%), Bankart lesions in 8 case (32%), free ALPSA lesion in 10 case (40%), bony Bankart lesions in 3 cases (12%), and adhesive ALPSA lesions in 1 case (4%). For the capsular lesion, the humeral avulsion of the glenohumeral ligament (HAGL) lesion was found in 2 cases (5%) and anterior capsular tear in 4 cases (10%). For SLAP lesions, type 1 was in 2 cases (5%), type 2 in 5 cases (12.5%), type 3 in 1 case (2.5%), with a total of 8 cases (20%). Among them, in 1 case the lesion was not observed in preoperative MRA screening. For bony lesions, Hillsachs lesion was discovered in 22 cases (55%), humeral greater tuberosity fracture in 4 cases (10%), and intraarticular loose body in 4 cases (11.1%). Among those cases of humeral greater tuberosity fractures, 2 cases coexisted with Bankart lesions, and 2 other cases with bony Bankart lesions. Rotator cuff lesion was found in 4 cases (10%). Among them, a partial articular side rupture was found in 2 cases (5%) and a complete rotator cuff tear in 2 cases (5%). Preoperative MRA did not pick up 1 of the type 2 SLAP lesion, and 1 case was classified as a type 3 under the arthroscopy. With the exception of these 2 cases, all the lesions coincided with preoperative MRA readings (94.4%).
Clinical results
Rowe's and Zarins' evaluation methods9 were used to analyze 25 cases showing anteroinferior labrum lesion. The average follow-up period was 18 months (range: 14 to 40 month). No periosteal rupture and displacement of labrum was found in 3 Perthes cases. Thus, no suture was performed. At the final follow-up, all 3 cases showed excellent outcomes. For 8 Bankart lesions, 7 were found to be excellent (87.5%), and 1 case in good condition (12.5%). Of the 10 free ALPSA lesions, excellent outcomes were found in 8 cases (80%) and good in 2 cases (20%). Excellent outcomes were found in 2 cases (66.6%) and fair in 1 case (33.3%) for 3 bony Bankart lesions found. The only 1 adhesive ALPSA showed a poor outcome. Of the total 22 cases that underwent arthroscopic suture, over 90 % of the patients showed results that were better than good.
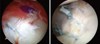
In 1 Bankart lesion and 1 adherent ALPSA lesion, a post-operative instability test resulted in a positive, and they eventually experienced recurrent dislocation. In 1 patient with a Bankart lesion, while playing basketball the patient's arm was caught on to other person's arm. The incidence resulted in hyperabduction of the arm and recurrent dislocation. The patient underwent a repeated operation (Fig. 1). The other patient rejected the suggestion of a repeated surgery. Post-operative infection or displacement of the screw was not seen. In 34 cases (94.4%), patients recovered and returned to sports activities comparable to the activity level before the injury. In 2 cases, the activity level was found to be reduced than before.
DISCUSSION
In young patients, acute anterior shoulder dislocation is recurrent in 50% of patients. Repeated shoulder dislocation and subluxation results in secondary damages to soft tissue, cartilage, humeral head, and glenoid bone. Prior studies based on surgery only reported intra-articular injuries almost in all cases of acute dislocation. In fact, the existence of intra-articular labrum lesion and, if it does, what type of lesions are present in patients without surgery is unknown. The authors recommended MRA to all the patients who came to the hospital due to acute anterior dislocation. If surgery is necessary, arthroscopic surgery was performed to discover the prevalence of accompanying lesions. Also, in what degree MRA readings coincide with actual findings of arthroscopy was studied.
Generally, Bankart lesions were considered core lesions in the anterior dislocation of the shoulder. However, in our study, prevalence of it was only 20%, which was much lower than the data reported in previous studies. It is difficult to compare this directly to other studies, since previous studies have not made detailed classifications of anteroinferior labrum lesions, such as the Perthes, Bankart, and ALPSA lesions like ours. However, our data suggested only a total of 62.5% of anteroinferior labrum lesions. Thus, it is difficult to define it as a core lesion in anterior dislocation.
Recently, to reduce recurrence, various approaches have been tried. For conservative management of the injury, Itoi, et al.1 suggested that external rotation of the humerus is more ideal for Bankart lesion reduction. The interpretation, they argued, is that the external rotation of the humerus applies tension to the anterior joint capsular membrane and therefore, it situates the Bankart lesion closer to the anterior glenoid rim. Seybold, et al.10 also argued that their average of a 12 month follow-up resulted in 10% recurrence and a higher functional score when applied at a 10 degree external rotation fixation for 3 weeks. However, for those under the age of 30 and active, conservative management involving internal rotation of a 4 to 6 week duration resulting in 80% to 90% risk of recurrence.6 Depending on the location of the fixation in conservative treatment, various outcomes can be reported. We believe the reason for the diversity of the outcomes is that authors in the past neglected the fact that a variety of anteroinferior labral lesions exists; we bundled up and classified various lesions mentioned in our study into the Bankart lesion only. This led them to a failure to report the outcome of conservative treatment depending on the types of lesions. Also, in our study, 2 cases of HAGL and 4 cases of a rupture of the anterior capsule were observed. This concludes that not all dislocations lead to a anteroinferior labrum lesion, and various types of anterior soft tissue damages such as HAGL lesion and capsular rupture can occur.
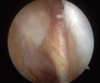
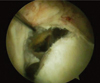
Preoperative MRA did not pick up 1 of the type 2 SLAP lesion and 1 case was classified as type 3 under arthroscopy. However, with the exception of these 2 cases, arthroscopic findings in all the lesions coincided with preoperative MRA readings (94.4%). We believe that MRA is an accurate method for assessing accompanying lesions. In fact, adherent ALPSA lesions (Fig. 2) or severely displaced Bankart lesions (Fig. 3) wereadhered and fixed by granulation tissue of the capsule membrane and coagulated blood on the inner side inferior of glenoid neck, and it is considered that, once the adhesion has occurred, it is difficult to distinguish two lesions under arthroscopy. However, with the high resolution provided by MRA, radiologists are able to further classify these lesions. Therefore, MRA helps surgeons and their patients get an idea of what injury was sustained after acute anterior dislocation of the shoulder. We believe that MRA is a reasonable modality to use to consult patients about a treatment method.
Arciero, et al.3 and Barber, et al.11 insisted that surgical treatment in acute anterior dislocation of the shoulder joint can enhance the quality of life by lowering high recurrence rates, protecting additional pathological transition of bone and soft tissue, and avoiding secondary morbidity of intra and extraartricular structure.
Recently, arthroscopic stabilization methods have produced outstanding results due to enhanced equipment, fluid transfer system, surgical technique, and aggressive physical therapy. Accordingly, many studies have been published about early surgical treatment's benefit to reduce complications and pain, recovery of exercise function, and relative lower incidence of recurrence than the non-surgical method. However, effects of the immediate surgical treatment option in the aspect of acute anterior dislocation of the shoulder are still debated.3,11,12
Both Bottoni, et al.13 and Kirkley, et al.14 presented encouraging data that showed favorable outcomes in an acute dislocation patient group of under 30 years old treated with the early arthroscopic stabilization method. Among the 25 cases showing anteroinferior labrum lesions, 22 cases, with the exception of 3 Perthes lesions, underwent arthroscopic repair and showed good results in 90% of patients according to Rowe and Zarins evaluation method. Perthes lesions were understood to be stable tissue, since it lacked periosteal damage or displacement of the labrum. Therefore, no suture was done to these lesions. At the follow-up, no signs of redislocation was found and clinical outcome was excellent. Also, the Bankart lesion, free ALPSA lesion, and bony Bankart lesion all showed excellent outcomes. Because the size of the study groups were small, further studies are recommended to find statistical significance among other lesions. The only case showing adhesive ALPSA lesion resulted in a poor outcome. Mobilization was attempted before apposition and reattachment during the arthroscopic procedure. However, full mobilization to the anatomical position was not accomplished due to adhesion at the inner side inferior of the glenoid neck.
Kim, et al.15 reported that, if a glenoidal defect accounts for more than 30%, the possibility of recurrent dislocation is very significant, and also reported that if the dislocation is associated with a Hill-Sachs lesion and capsular laxity, these are known risk factors to raise the post-operative recurrent risk of instability. Regardless of specialties, the most important factor that leads to a successful operation lies in choosing the right surgical method for the right patient. Thus, we screened patients with MRA and CT before the operation to exclude patients with risk factors that can raise incidence of recurrence. Those who had evidence of multidirectional instability or had over 25% glenoidal defect were eliminated as possible candidates of immediate arthroscopic stabilization.
Immediate arthroscopic stabilization gives patients the opportunity of fast and full recovery that enables an early return to daily activities. However, it is important to consider the high cost of the method and complications associated with the surgery. Also, it is important to consider that performing arthroscopic stabilization appears to be an overtreatment, if a patient's condition can fully recover with conservative measures only. Therefore, when planning to treat acute anterior dislocation of the shoulder, detailed preoperative examinations are required to pinpoint the most efficient treatment modality.
Several limitations in our study exist. First, the study was composed of a relatively small number of subjects. Second, the average follow-up period was brief. Finally, our study did not have a control group.
In conclusion, under MRA and arthroscopy performed on patients with acute anterior shoulder dislocation, it was observed to have varying types of anteroinferior labrum lesions such as Perthes, Bankart, ALPSA, and bony Bankart lesions. MRA is a remarkably useful tool in classifying various lesions in acute anterior dislocation of the shoulder and to make a diagnosis, making it a useful tool to decide a treatment method while consulting with patients and their families.
 XML Download
XML Download