

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
It is well known that chronic hyperglycemia is a major contributor to microvascular complications. Diabetic nephropathy is one of the most serious microvascular complications and leading cause of mortality and morbidity in diabetic patients. There are several mechanisms of diabetic nephropathy including the activation of protein kinase C (PKC), increased advanced glycosylation end products, the upregulation of cytokines and growth factors, and activation of rennin angiotensin system.1-4 These mechanisms are known to participate in the increase of renal vascular endothelial growth factor (VEGF) production.5-9
It has been reported that VEGF is a mitogenic factor for vascular endothelial cells and involved in vasopermeability.10 Recent data showed that VEGF gene expression increased in diabetic kidneys and could be reduced by VEGF antibodies or angiotensin receptor blockers (ARB).6,11-14 So, it has been considered that VEGF may be an important factor in the progression of diabetic nephropathy and regulation of VEGF expression is a potential therapeutic target for treatment of diabetic nephropathy.
Intracellular hyperglycemia activates the polyol pathway, which is one of the pathogenic pathways involved in diabetic microvascular complications.15,16 Aldose reductase (AR) is the key enzyme that catalyzes nicotinamide adenine dinucleotide phospate (NADPH) in the polyol pathway, which eventually leads to the reduction of glucose to sorbitol.15 It was reported that increased AR activity derived from hyperglycemia could induce retinal VEGF overexpression and administration of fidarestat, a highly specific AR inhibitor (ARI), could ameliorate retinal VEGF expression in a diabetic rat model.17
In this study, we investigated the effects of ARI on diabetic nephropathy and renal VEGF expression in a type 1 diabetic rat model and compared the effects with angiotensin receptor blocker which could reduce renal VEGF expression.
MATERIALS AND METHODS
Animals
Eight-week-old male Sprague-Dawley rats weighing 200-250 g were purchased. At nine weeks of age, diabetes was induced by a single injection of streptozotocin (70 mg/kg body weight) into the intraperitoneum. One week later, rats with glucose levels higher than 200 mg/dL were considered diabetes mellitus. The experimental rats were divided into four groups, including a normal control group (CON, n = 6), a diabetic control group (DM, n = 10), a fidarestat treated diabetic group (DM + ARI, 16 mg · kg-1 · day-1, n = 10), and an angiotensin II receptor blocker treated diabetic group (DM + ARB, losartan, 20 mg · kg-1 · day-1, n = 10) as a positive control. Fidarestat was administered via a standard diet, while losartan was administered by orally through a gavage tube from 9 to 32 weeks of age.
We monitored body weights monthly and blood glucose levels (Surestep®, Lifescan Inc., Milpitas, CA, USA) from the tail vein weekly. Twenty four hours urine was collected for assessment of albumin (Roche Molecular Biochemicals, Indianapolis, IN, USA) and creatinine levels at 8 and 32 weeks of age.
Kidney extraction
At 33 weeks of age, rats were anesthetized with ketamine hydrochloride (70 mg/kg) by intraperitoneal injection and both kidneys were extracted. One kidney was preserved using a quick freeze method with liquid nitrogen while the contralateral kidney was fixed in 4% paraformaldehyde for 48 hours, and then embedded in paraffin for histological examination and immunohistochemical staining of VEGF.
Measurement of glomerular volumes and mesangial matrix index
Paraffin embedded tissues were cut into 5 µm thick sections and stained with periodic acid-Schiff (PAS) stain. We examined these sections with an optical microscope that was equipped with a charge coupled device camera (Pulnix, Sunnyvale, CA, USA) in order to obtain pictures of glomeruli, which were subsequently sent to a computer monitor. We measured 40 glomerular areas per rat using an image analysis system (GmbH, SIS, Minster, Germany). In addition, we calculated glomerular volume by the Weibel and Gomez formula:18 Glomerular volume (Gv) = Area1.5×1.38/1.01 (1.38: shape coefficient, 1.01: size distribution coefficient).
Glomerular matrix index was assessed in 40 glomeruli per each rat after locating the slices on the center of the camera and scored as grade 0 to 4: grade 0, normal glomeruli; grade 1, mesangial expansion area up to 25%; grade 2, 25% to 50%; grade 3, 50% to 75%; grade 4, 75% to 100%; estimated and put into 0 to 4 scale.19 A kidney slide was assessed 10 times.
Calculation of optical density of VEGF
After paraffin embedded tissues were cut into 5 µm-thick slices, they were placed on slides and the paraffin was removed in order to carry out immunohistochemical staining. Shortly after paraffin removal, the slides were transferred into a 10 mm/L citrated buffer solution (pH 6) and washed with distilled water. The slides were then immersed in a 0.05% H2O2-methanol solution for 15 minutes, and were then placed in an anti-VEGF antibody solution (Santa Cruz Biotechnology, Inc., California, CA, USA), which was diluted 1 : 1000 at room temperature. The slides were then processed with a biotinylated secondary antibody using a Rat ABC staining system (Santa Cruz Biotechnology, Inc., California, CA, USA) and avidin-biotinperoxidase complex (ABC reagents). Finally, the slides were incubated with peroxidase substrates, which included 0.05% 3, 3'-diaminobenzidine tetrahydrochloride (DAB).
We investigated the stained tissues using the same optical microscope setup described above (Pulnix, Sunnyvale, CA, USA). We measured the optical density of stained VEGF using an image analysis system (GmbH, SIS, Minster, Germany).
RNA extraction and preparation of cDNA
Total RNA was isolated from the frozen kidney tissues using TRIzol reagent (Invitrogen Life Technologies Inc., Gaithersburg, MD, USA) as described in the product manual; the amount of RNA obtained was determined by spectrophotometry. A total of 1 µg of RNA was mixed with 500 µg/mL oligo d(T)15 primer, 200 U/mL of moloney murine leukemia virus (MMLV) reverse transcriptase (RT), 10 mM dNTPs, 40 U/µL RNase inhibitor, and MMLV RT 5× buffer (Promega, San Luis Obispo, CA, USA) to make a final reaction volume of 25 µL. The mixture was incubated at 42℃ for 30 min and the reaction was terminated by raising the temperature to 95℃ for 5 min. Reverse transcriptase-polymerase chain reaction (RT-PCR) reactions were carried out via automatic thermocycling (MJ Mini Thermal Cycler, BIO-RAD, Hercules, CA, USA).
Real time RT-PCR for VEGF
Prepared complementary DNA (cDNA) and primer of rat glyceraldehyde-3-phosphate dehydrogenase (GAPDH) or VEGF were mixed with 10× QuantiTect Primer Assay (Qiagen, Valencia, CA, USA) and a Syber Green RT-PCR kit (Qiagen, Valencia, CA, USA). Samples were subjected to real-time RT-PCR using a Roter-Gene RG-3000 cycler (Corbett Research, Mortlake, NSW, Australia). The Syber Green RT-PCR conditions were as follows: 15 sec at 94℃, 30 sec at 58℃, and 30 sec at 72℃, with the total number of cycles ranging from 40 to 45. Data was analyzed with the software provided by Roter-Gene. Syber Green Ct values were determined using GAPDH normalization. To avoid contamination, all assays were performed according to universal thermal cycling parameters and all experiments were performed in triplicate.
RESULTS
Clinical characteristics in experimental animals
At eight weeks of age, there was no difference in body weight between the control and diabetic groups (all rats had body weights of 200-250 g). However, body weights were significantly lower in the diabetic control, as well as all of the medication treated diabetic groups, when compared with the normal control group at 32 weeks of age. Blood glucose levels increased approximately 4 to 5 fold in diabetic rats compared with control rats. There were no statistically significant differences between untreated diabetic and ARI or ARB treated diabetic rats with respect to blood glucose concentration (Table 1).
Changes of 24 urinary albumin levels and ACR
At 8 weeks of age, 24 hour urinary albumin excretion and albumin creatinine ratios (ACR) were not different among the experimental rat groups. At 32 weeks of age, a progressive increase of 24 hour urinary albumin and ACR were observed in all rat groups compared with those of the 8 weeks. In the fidarestat and losartan treated groups, 24 hour urinary albumin excretion and ACR were significantly lower than that of the diabetic rat group at 32 weeks (ACR: DM + ARI; 9.96 ± 10.68, DM + ARB; 6.61 ± 9.05, DM; 84.85 ± 91.19 mg/gCr). The decrease of ACR was approximately 64% of the ARI treated DM group and 81% of the ARB treated DM group compared with the diabetic control group (Table 2).
Glomerular volumes and glomerular matrix index
Although the calculated glomerular volumes did not show significant differences among the experimental groups, glomerualr mesangial expansion was observed in the DM group compared with other groups in PAS staining of glomeruli (Fig. 1). Also, glomerular matrix index (GMI) scores significantly decreased in the CON group (1.05 ± 0.05) and all medication treatment groups (DM + ARI; 1.088 ± 0.153, DM + ARB; 1.075 ± 0.175, p < 0.001 vs. DM group) compared with the DM group (2.1 ± 1.122) (Fig. 2).
Renal VEGF expression
In the DM group, immunohistochemical stain for VEGF in the kidney showed darker brown pigmentation than other groups (Fig. 3). Compared with the CON group, the optical density of immunohistochemical staining for renal VEGF in the DM group significantly increased and restored in ARI and ARB treated rat groups (Fig. 3).
Renal VEGF mRNA expression
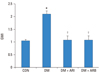
For quantification of renal VEGF mRNA expression, we examined real time RT-PCR. The VEGF/GAPDH ratio was 8.32 fold in the DM group, 1.52 fold in the DM + ARI group, and 1.35 fold in the DM + ARB group compared with the CON group. The ARI treatment decreased VEGF mRNA expression by 82% compared with the DM group. Significant differences in VEGF mRNA expression between the ARI and ARB treated diabetic groups were not observed (Fig. 4).
DISCUSSION
In this study, we found that aldose reductase inhibitor, fidarestat, could reduce the albumin excretion by ameliorating the VEGF expression in streptozotocin-induced diabetic rats as like angiotensin receptor blocker, losartan.
Diabetic nephropathy is the most serious complication of diabetes, and is the most common cause of end-stage renal disease. During the early phase of diabetic nephropathy, glomerular hyperplasia and thickening of glomerular basement membranes with mesangial protein accumulation may appear.3 These processes could lead to glomerular hyperfiltration and microalbuminuria initially, and eventually progress to renal failure and end stage renal disease.20 Many factors contributed to these processes such as advanced glycation end products, PKC activation, transforming growth factor-β, and other growth factors.2,11,21 In addition, it has been demonstrated that AR activity increased in diabetic nephropathy.22 There is a positive relationship between the severity of glomerular structural changes and the immunoreactivity of AR.23 Donnelly, et al. reported that tolrestat could prevent glomerular hyperfiltration and extracelluar matrix accumulation in streptozotocin-induced diabetic rats.24 Furthermore, Isogai, et al.25 demonstrated that epalrestat could rescue glomerular basement membrane shrinkage and reduce urinary albumin excretion in a diabetic rat model.
In this study, the glomerular volume was not different among all experimental groups, but mesangial expansion was observed in the diabetic control group compared with the normal control and medication treated rat groups. This data could be explained by glomerular sclerosis because glomerular sclerosis might be derived from long term hyperglycemic conditions. However, we could suggest that fidarestat could affect the renal structure by decreasing mesangial expansion.
AR activity may induce diabetic nephropathy by several mechanisms such as increased lipid peroxidation, depletion of major nonenzymatic antioxidants, and downregulation of superoxide dismutase activity.21,26-28 The polyol pathway which is activated by hyperglycemic conditions may increase the production of superoxide - and nicotinamide adenine dinucleotide - induced reactive oxygen species (ROS), and could enhance VEGF mRNA expression.29
Various data has shown that VEGF expression is increased in diabetic rat models and administration of anti-VEGF antibodies to diabetic rats could suppress urinary albumin excretion by reducing hyperpermeability, glomerular basement membrane thickness, and mesangial expansion.12,13,30 There were many factors that could increase VEGF levels. It is known that various cytokines and growth factors including transforming growth factor-β reactive oxygen species, and activation of rennin-angiotensin system could increase renal VEGF expression.1-4 Previously, we demonstrated that diabetic nephropathy could be improved by treatment of theangiotensin receptor blocker by decreasing renal VEGF expression.14 For these reasons, VEGF is thought to be an important factor in the development of diabetic nephropathy.
In the present study, we showed that 24 hour urinary albumin creatinine ratio (ACR) and renal VEGF expression were significantly increased in diabetic rats and fidarestat treatment could improve the diabetic nephropathy concordance with decreasing renal VEGF expression similar to losartan treatment. Our data could suggest that fidarestat could improve diabetic nephropathy by reducing renal VEGF expression.
The first discovered aldose reductase inhibitor, tolrestat, was withdrawn because of the side effects of hepatic necrosis.31 In our experiment, the fidarestat feeding diabetic rats all survived. In spite of our data, a safety profile should be provided in future studies.
In this study, losartan was used as a positive control. It has been reported that VEGF expression could be inhibited by treatment with ARB.14,32 Our data showed that the ability of VEGF reduction did not distinguish between fidarestat and losartan treated rat groups, indicating that fidarestat could affect the prevention of diabetic nephropathy.
In conclusion, our findings suggested that fidarestat treatment could improve the diabetic nephropathy by reducing renal VEGF expression in type 1 diabetic rat model. Further clinical studies should take place for the establishment of fidarestat treatment in diabetic nephropathy.




 XML Download
XML Download