

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Accidental exposure to small amounts of caustic substances occurs most frequently in children.1,2 The early manifestations of such exposures are abdominal pain, nausea, vomiting, hoarseness, and dyspnea due to injury of the upper airway. The systemic symptoms of caustic injuries include fever, tachycardia, tachypnea, and shock; the late development of dysphagia, due to stricture formation, can lead to weight loss and malnutrition.3-5 Esophageal dilatation has been the primary treatment of esophageal strictures.6 Many patients with esophageal strictures have recurrence of symptoms after dilatation.3 Surgical intervention has been carried out in patients with chronic esophageal strictures who require repeated dilatation or fail dilatation therapy.7 However, balloon dilatation or endoscopic bougienage is still necessary for the recurrence of strictures after surgery. These procedures are invasive and expensive, especially when they are performed repetitively. Self-bougienage may be a useful alternative to surgical treatment or repeated endoscopic dilatation in patients with recurrent benign esophageal strictures and postoperative dysphagia with esophageal stricture, particularly in those patients who are poor surgical candidates.8,9
The objective of this study is to assess the long-term effects on the esophagus of dilatation therapy and surgery for caustic ingestions, and to evaluate the efficacy of self-bougienage for refractory esophageal strictures after surgery.
MATERIALS AND METHODS
From May 2000 to May 2008, we treated nine cases of severe esophageal stricture after a caustic injury to the esophagus. They were treated by endoscopic balloon dilatation, bougienage, or surgery at Samsung Medical Center, Seoul, Korea. We reviewed the medical records of all cases retrospectively. The parameters examined included age, gender, caustic agent, site and length of the stenosis, onset of the stenosis, effectiveness and outcome of the balloon catheter dilatation, endoscopic bougienage, and surgical treatment. Two months after the caustic ingestion, a barium esophagogram was performed in all patients to evaluate the location and general contour of the stricture.
Endoscopic bougienage or balloon catheter dilatation was performed for patients who had an esophageal stricture with severe dysphagia. Endoscopic bougie dilatation was performed with the Savary-Gilliard dilators (Cook Medical, Bloomington, IN, USA). Dilators with 7-, 9-, 10-, or 11-mm-diameters were inserted under endoscopic guidance. Thereafter, dilation was performed under fluoroscopic control. Each treatment session consisted of two or three dilations, with the size of the dilator increasing incrementally by no more than 3 mm. After the final dilation, endoscopy was performed to access the efficacy of the dilatation as well as complications such as bleeding or perforation of the esophagus. Balloon catheters were used in patients with a long stricture with a minimum of 6 mm to a maximum 16 mm diameter under fluoroscopic control. The balloon was slowly inflated with normal saline to specified pressures for each balloon and maintained for one minute and then deflated. The procedure was repeated two or three times with a larger sized balloon until an effective dilatation was obtained without complications. After the dilation procedures, the patients fasted for 12 hours. The treatment was considered effective when patients were able to eat solid or semisolid foods without dysphagia.
In this study, there was one case with long and rigid strictures that were not suitable for dilatation; esophageal replacement with gastric transposition was performed as the first-line treatment. The other patients received endoscopic bougienage or balloon catheter dilation. If repeated dilations were not effective, surgery was considered for second-line treatment. The surgical procedure was decided by the extent and location of the esophageal stricture. Esophageal replacement and end to end anastomosis, esophageal replacement with gastric transposition, or esophageal replacement with colon interposition were performed in seven of the nine children. When an anastomotic site stricture developed, we recommended endoscopic bougienage, balloon catheter dilation, or self-bougienage according to the patient's compliance. For self-bougienage, the parents were taught the following technique at the outpatient clinic. A dilator with a 10-11 mm diameter was first lubricated with tap water, and the tapered end was then introduced into the pharynx to the stomach. The dilator was kept in place for one minute and then removed. We explained to the parents that the potential complications of esophageal dilatation included aspiration, perforation, hemorrhage, and bacteremia. Before the first self-bougienage, a preliminary dilatation and endoscopy was performed by a physician under fluoroscopic guidance. The parents performed bougienage at home once a day for the first three months, one time every two to three days for the next three months, once a week for the next three months, and then once a month, or if the children were not able to eat solid or semisolid foods.
RESULTS
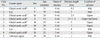
There were nine patients with esophageal strictures after caustic injuries. The group consisted of six males and three females with a mean age of 30 months (range 22 to 79 months). Six patients had a history of strong acid ingestions, two strong alkaline, and in one the agent was unknown. All of these cases involved accidental ingestion of concentrated caustic agents. The mean time from the initial injury to severe esophageal stricture, defined by the inability to swallow solid or semisolid food, was four weeks (range, 1 to 8 weeks). The location of the esophageal stricture was the upper esophagus in five, the mid esophagus in four, and multiple sites in one. The mean length of the esophageal stricture was 3.8 cm (range, 1 to 9.2 cm). Four patients had a long segment stricture (longer than 5 cm) and one patient had multiple strictures (Table 1).
One patient had surgical treatment without dilatation procedures. Eight patients received repeated dilatations using a balloon catheter or a bougie catheter. Among the eight patients, two patients had complete resolution of their symptoms and six patients required surgery. Two of the nine patients had complete resolution of their symptoms with repeated dilatations, seven of the nine patients required surgery (Fig. 1). One patient had a short segment stricture and required surgery due to perforation during the first trial of bougie dilatation.
Nine patients were followed during an average of 60 months (range, 12 to 96 months). The interval between the caustic ingestion and the esophageal surgery was on average 19 months (range, 2 to 48 months). The mean intervals between surgery and developing a stricture recurrence at the esophageal anastomotic site, requiring balloon dilatation or bougienage, was 12 months (range, 2 to 40 months) (Table 2). Among the five patients that developed stricture recurrence of the esophageal anastomotic site, three had improved symptoms by self-bougienage and two had improved symptoms by repeated balloon dilatation or bougienage; there were no complications in these patients.
DISCUSSION
Treatment of esophageal strictures is directed at curbing the symptoms of dysphagia, avoidance of the complications of esophageal obstruction, and the prevention of the recurrence of the strictures.3 In this report, as primary treatment for an esophageal stricture, eight of the nine patients had endoscopic bougienage or balloon catheter dilatation performed; there was one exception due to a severe long segment (9.2 cm) esophageal stricture. Four of the five cases with a long segment stricture (more than 5 cm) or multiple strictures had a recurrence of the strictures after surgical treatment; in these cases self-bougienage was recommended as an alternative treatment to reduce invasiveness and cost compared to the conventional procedures.
To our knowledge, few studies have been reported on the self-bougienage in children with caustic esophageal strictures. Gündoğdu, et al.10 reported that the success of bougie dilatation was higher in patients younger than eight years of age, in strictures caused by caustics other than lye, involving the upper third portion of the esophagus, and less than 5 cm in length. In our report, two patients that improved with only dilatation therapy, without surgery, fit the above criteria. Among the seven patients that required esophageal surgery, five had stricture recurrence at the anastomotic site after surgery. Two of them had improved symptoms after one to two endoscopic bougienage or balloon dilatation procedures, and three had improvement with self-bougienage.
Gilmore and Sheers11 reported positive outcomes with self-bougienage in two patients requiring frequent dilations. Kim, et al.9 reported on seven patients who had recurrent benign esophageal strictures treated with self-bougienage; they noted long-term symptomatic relief in the patients after self-bougienage. Dilatation therapy requires frequent admissions to the hospital and multiple procedures with anesthesia with the inherent associated risks. Therefore, self-bougienage might be a safe and practical approach to restenosis after esophageal resection with anastomosis in a subset of patients who require frequent dilatation to maintain esophageal patency. In our experience, home bougie dilation of esophageal strictures was well tolerated and reduced the need for regular endoscopic management in patients with recurring problems. Patients who performed self-bougienage experienced little discomfort from the procedure. Self-bougienage is cost-effective and safe with adequate patient instruction and periodic physician follow-up.8 In this study, the three patients who performed self-bougienage were more comfortable with the bougie at home than the dilatation procedures at the hospital. However, although none of our patients experienced complications, self-bougienage has the risk of esophageal perforation and therefore candidates must be selected carefully.3
The strong limitation of this study is the single center review with a very small number of patients. Therefore, it may not be enough for us to draw conclusions from our study results. In our experience, however, self-bougienage was a safe, less invasive, and effective alternative treatment for esophageal strictures in carefully selected children with good compliance. Confirmation of the safety and effectiveness of self-bougienage in children now requires a multicenter trial.


 XML Download
XML Download