

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A hydatid cyst is a parasitic disease that is frequently encountered in the sheep and cattle-raising regions of the world, and has been most frequently observed in Australia, New Zealand, South Africa, South America, Mediterranean countries, Asia, and Africa. The presence of pulmonary hydatid disease should be considered in patients that present with a well-defined, spherical density of the lung, particularly in those who have lived or traveled in endemic areas. According to previous knowledge, if a giant pulmonary hydatic cyst occupies more than 50% of the pulmonary lobe it can be removed by a lobectomy. However, in the present case, while the cyst occupied more than 90% of the lobe, it was not excised by a lobectomy, so that the remaining lung tissue could be preserved.1 Hydatid cyst disease is also an important public health and socio-economic problem in our country, Turkey.2
CASE REPORT
A 20-year-old female, who had a cough, chest pain, and dyspnea was admitted to our department. Her complaints had progressively increased within the days prior to admission. A physical examination revealed no chest wall movements or pulmonary sounds on the left wall of the patient' chest, with a tentative diagnosis of pleural effusion initially made (Fig. 1).
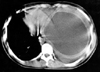
The material obtained by fine needle aspiration was examined by light microscopy, prepared directly by wet mount after centrifugation at the parasitology laboratory. The sample showed protoscoleces and hooklets. Computed tomography of the chest, and posteroanterior and lateral chest radiography were performed. The computed tomographic scan showed a giant cyst (33×14×12 cm), which pushed the heart to the right side and completely involved the left thorax (Fig. 2).
Operative techniques
The patient was placed in the lateral decubitus position under general anesthesia. The pleural cavity was entered through a left posterolateral thoracotomy at the fifth intercostal space. The fluid of the hydatid cyst was first aspirated from the top of the cyst, with a 20-gauge needle to reduce the intracystic pressure. Later, a suction apparatus was placed into the cyst to ensure complete aspiration of the fluid. The germinative membrane was excised from the cyst by widening the needle insertion site (cystotomy). After removal of the remnants of the germinative membrane, the residual cavity was carefully cleaned and reexamined for the presence of possible daughter vesicles, and then the pericystic cavity was washed with 1% povidone-iodine solution. During the operation period only 5% of the pericystic tissue was extracted. The cavity was obliterated with pure-string absorbable sutures, starting from the bottom (capitonnage), after all the bronchial openings had been carefully closed with closer and deeper sutures. The atelectatic apical lobe was freed and expanded. Following placement of chest tubes into the apical and costophrenic regions of the pleural space, the thoracotomy was closed.
The costophrenic chest tube was removed on the first postoperative day. Because of problems with prolonged air leakage and unexpansion, a control computed tomography was performed on the 7th postoperative day. At the end of this investigation a pleural space was determined in the anterior region. For this reason, the pezzer tube was placed under local anesthesia in the anterior second intercostal space for drainage: at the same time the apical chest tube was withdrawn from the costophrenic region. Later, the costophrenic chest and the pezzer tubes were removed on the 11th and 13th postoperative days, respectively. The patient was discharged, with a minimal pericardiac aseptic pleural space, on the 14th postoperative day (Fig. 3).
During the postoperative period, in order to prevent the recurrence and occurrence of a secondary cyst, chemotherapy (albendazole) at a dose of 10 mg/kg/day was used for 6 weeks. After two months, when the patient returned for control, the left lung was observed to have completely expanded on the posteroanterior and lateral chest radiography. No recurrence was encountered within three year follow-up period.
DISCUSSION
The clinical manifestations of hydatid cysts depend on the site and size of the cyst. Small, peripherally located cysts are usually asymptomatic, whereas large cysts may manifest with symptoms of compression of the adjacent organs. Most pulmonary hydatid cysts may remain asymptomatic for a long time until they grow large enough to cause signs and symptoms, such as a nonproductive cough, chest pain, and dyspnea. Complications, such as rupture, secondary infection, pneumothorax and suppuration may sometimes precede the diagnosis.3
The current treatment for a pulmonary hydatid cyst is complete excision of the part involving the hydatid cyst, with maximum preservation of lung tissue.1,4 Although surgery remains the treatment of choice for hydatid disease, the usefulness of drug therapy has been reported in many studies. Mebendazole, and more recently albendazole, have been used as primary drug therapy and as a drug adjunct to surgery to diminish the recurrence and potential spread of the organism.5,6
Cystotomy, with capitonnage, has been the most commonly applied operative procedure in the literature.7 The optimal surgical approach is still a matter of controversy. The optimal procedure for most cases of lung hydatid cysts is cystotomy followed by capitonnage. As opposed to pericystectomy or enucleation (removal of the endocyst without previous puncture), cystotomy minimizes the risk of an uncontrolled intraoperative rupture. Rupture can result in anaphylactic shock or dissemination. Enucleation should only be performed in cases of small (< 4 cm) and unruptered cysts.8 On the other hand, one of the principal indications for a lobectomy is a large cyst involving more than 50% of the lobe.1 Although, the cyst in our case involved more than 90% of the left-lower lobe, no lobectomy procedure was applied, and the atelectatic lobe was completely expanded. In our view, even if pulmonary hydatid cysts involve more than 50% of the lung lobe, a lobectomy must be avoided as far as is possible. However, a lobectomy procedure must be performed in complicated cases, such as severe suppuration, multiple unilobar cysts and severe hemorrhage.


 XML Download
XML Download