

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A nevus is a benign melanocytic neoplasm and is the most common type of skin tumor.1 It may occur anywhere on the skin, but its appearance in the external auditory canal (EAC) is very rare. So far, fewer than 20 cases of nevus in the EAC have been reported in the English literature.1-5 Dysplastic nevi are characterized by an increased number of predominantly nested melanocytes in the basal epidermis, random cytological atypia, elongated and fused rete ridges, architectural atypia and stromal changes.6 Although the concept of dysplastic nevi remains controversial, their clinical significance has been widely accepted. Dysplastic nevi are important as potential precursors for melanoma and simulants of melanoma.6,7 A melanocytic nevus is usually treated for cosmetic purposes, but dysplastic nevus is treated to exclude a diagnosis of melanoma or to prevent possible malignant transformation.7 Therefore, recognition of dysplastic nevi is significant for proper management. Dysplastic nevi may be identified by clinical observation, but it is hard to thoroughly inspect nevi within the EAC.
Here, we describe a patient with a dysplastic nevus in her EAC, which caused a conductive hearing loss. The mass showed clinically characteristic findings of a melanocytic nevus, but there were components of a dysplastic nevus in the medial portion of the nevus. To our knowledge, this is the first reported case of a dysplastic nevus in the EAC within the English literature.
CASE REPORT
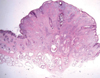
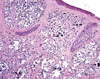
A 33-year-old woman presented with a one-year history of feeling blockage in her left ear. She denied otorrhea, otalgia, dizziness, previous otologic surgery and trauma. Physical examination revealed a protruding mass arising from the posterior wall of the left ear canal's cartilaginous portion (Fig. 1). It was a dark brown, nontender, dome-shaped, haired mass which partially occupied the EAC. The tympanic membrane was not visible due to the mass. Audiologic examination revealed normal hearing on the right and conductive hearing loss on the left. The four-frequency pure tone average was 30 dB for air conduction and 10 dB for bone conduction. The patient underwent excisional biopsy via a transcanal approach under local anesthesia. An elliptical incision was made around the mass with adequate margins under microscopy. A deep margin was taken to the level of the perichondrium. The surgical specimen, which measured 1.0 × 1.0 × 0.8 cm, was a spherical mass confined to the cartilaginous EAC and consisting of multiple polypoid and brownish tissue fragments. After the mass was excised, the surgical wound was closed with non-absorbable suture material. The mass was subjected to histopathologic assessment, which revealed normal skin covering the specimen and numerous nests and groups of melanocytic nevus cells located in the dermis (Fig. 2). These findings were compatible with an intradermal nevus, but the nevus contained atypical melanocytes without pleomorphism (Fig. 3). Therefore, the final diagnosis was a dysplastic nevus within an intradermal nevus.
Following surgical excision, the patient experienced an uneventful recovery. There was no evidence of recurrence two years after operation and the patient's hearing was normal.
DISCUSSION
A dysplastic nevus is typically a macular lesion 6 mm or more in diameter, usually with irregular, fuzzy borders.8 Dysplastic nevi may be present anywhere on the skin, but appear mostly on the upper back. The risk of melanoma in people with dysplastic nevi increases with an increasing number of nevi and with a personal or family history of melanoma. The presence of dysplastic nevi is an independent risk factor for the development of multiple primary melanomas.7 Dysplastic nevi may be confused with melanomas both clinically and histologically. Clinically, dysplastic nevi share many features with melanomas, including asymmetry, border irregularity, color variability and a diameter greater than 6 mm.9 Histologically, dysplastic nevi are characterized by both specific cytologic and architectural abnormalities. Cytologically, a minority of the cells in dysplastic nevi exhibit atypia, which is characterized by nuclear enlargement, slight irregularity and hyperchromasia.7 Despite the recognized association between dysplastic nevi and the risk of melanoma, the majority of dysplastic nevi never progress to melanoma.8 However, when melanoma cannot be ruled out after careful examination or when there are changes in a dysplastic nevus or findings for suspicion of melanoma, an excisional biopsy is recommended. Correct diagnosis cannot be made until excision and pathological examination are done.
In our case, the mass in the ear canal showed characteristic findings of a melanocytic nevus which is considered as a benign cutaneous tumor, and is a collection of groups of melanocytic nevus cells located in the epidermis, dermis and rarely, subcutaneous tissue. Melanocytic nevi usually arise within the first few decades of life and, as the person ages, decrease and are replaced by fibrosis. Melanocytic nevi may clinically show five distinct types: flat lesions, slightly elevated lesions, papillomatous lesions, dome-shaped lesions and pedunculated lesions.2 In our case, the nevus was a dome-shaped papular lesion arising from the cartilaginous ear canal's posterior wall. The posterior and inferior EAC walls were the most common sites of melanocytic nevi in a previous report.1 Most papillomatous lesions and almost all dome-shaped and pedunculated lesions represent intradermal nevi.2 Melanocytic nevi have histologically been classified into three subtypes: junctional nevi, in which the nevus cells are confined to or remain in contact with the lower epidermis; intradermal nevi, in which the nevus cells are located within the dermis and no longer contact the epidermis; and compound nevi, which display the features of both junctional and intradermal nevi.2 Histologically, our case was an intradermal nevus, but also showed the presence of atypical melanocytes without pleomorphism within the nevus. Usually, the risk of a single melanocytic nevus transforming into a cutaneous melanoma is very low, however, dysplastic nevi are known as possible precursors of melanoma.7,10 The gross appearance of our case indicated a common melanocytic nevus, but an atypical component was scattered in the whole portion of the nevus. It was impossible to histologically observe the medial portion of the nevus, therefore, we planned to pathologically confirm the nevus. We believe that it is important to pathologically confirm all nevus-looking masses within the EAC by excisional biopsy when a nevus becomes symptomatic or when all of its features cannot be observed. The possibility of malignancy should be excluded.

 XML Download
XML Download