

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Atrial fibrillation (AF) is an important arrhythmia because it is associated with an increased risk of systemic thromboembolism and stroke. The attributable risk for stroke associated with AF increases steeply from 1.5% at age 50 - 59 years to 23.5% at age 80 - 89 years.1
Five large randomized controlled primary prevention trials and meta analysis study have shown that warfarin reduced the risk of stroke by about two thirds in people with non-valvular AF (NVAF), from overall 4.5% to 1.4% per year with little increase in frequency of major bleeding or intracranial hemorrhage.2-7
Advancing age, prior stroke or transient ischemic attack, diabetes mellitus (DM), hypertension, dilated left atrium, and impaired function of the left ventricle are known risk factors for thromboembolic event.8-12
Warfarin has been found to be effective for primary and secondary prevention of ischemic stroke, reducing the risk by 68% and the mortality by 33%.13 However, there are several problems in warfarin treatment which include narrow therapeutic range, much inter and intra individual variation, exorbitant price for antithrombotic effect, about a 4 day lag effect and essential monitoring.
The purposes of this observational study were to assess the degree of OAC in patients with NVAF, who were treated with warfarin, using new index which we made and evaluate the correlation between INR stability and thromboembolic events.
MATERIALS AND METHODS
Study population
This study included 129 patients with chronic NVAF who were treated with warfarin prior to conducting this study from April 2000 to December 2005. All patients were diagnosed as NVAF by an attending cardiologist at Samsung Medical Center.
NVAF was defined as an atrial fibrillation without any stenotic valvular heart disease (VHD), ischemic heart disease and more than mild regurgitant VHD.
We analyzed the following parameters for each patient: age, gender, dates of thromboembolic event and the INR values, dates of bleeding episode and INR values, and alcohol intake. In addition, known risk factors for stroke (past cerebrovascular attack or transient ischemic attack, hypertension, congestive heart failure, and DM) were assessed, and left atrial diameter as well as left ventricular ejection fraction were estimated by transthoracic echocardiography. A CHADS2 score (congestive heart failure, hypertension, age > 75 years, diabetes, and previous stroke or transient ischemic attack) which ranged from 0 to 6 was calculated for each patient. Patients were assigned points as follows: history of congestive heart failure = 1 point, history of hypertension = 1 point, age > 75 years = 1 point, history of diabetes mellitus = 1 point, and history of stroke including transient ischemic attack or systemic embolism = 2 points.14
All patients were registered at the anticoagulation service. Anticoagulation service was regarded as a mechanism to improve the provision of anticoagulation. The rationale for anticoagulation service is that the day-to-day details of anticoagulation management are delegated from busy physicians to an anticoagulation service manager (typically, a pharmacist, nurse or nurse practitioner), who is responsible for dosing changes, scheduling patient education, and other aspects of anticoagulation management. When INR values are not within the therapeutic range, all possible reasons were recorded by the anticoagulation service. It was validated by an on-line database (Micromedex®).
When initiating warfarin therapy, warfarin should usually be initiated with a 4 mg dose (or 2 to 3 mg in the very elderly). Adjusting a steady-state warfarin dose depends on the INR values measured and clinical factors. The total weekly dose should be changed by 10% to 20% for the most. The INR should be monitored frequently (e.g., at least once a week) immediately after initiation of warfarin. Subsequently, the interval between INR tests can be lengthened gradually (up to a maximum of 8 to 10 weeks) in patients with stable INR values.
INR stability
It was defined as a percentage of the value derived by dividing the number of INR within the target range by total number of INR measurement after first achievement of adequate INR range. In cases that subjects' INRs are out of the target range, repetitive INR measurements were performed for relatively short time period. Therefore, we excluded the INR values from measuring INR stability when the time period between any two consecutive measurements was less than 2 weeks.
Subgroups
The subjects were divided into 2 subgroups to evaluate the relation between INR stability and clinical outcomes. One group was patients who suffered from stroke or thromboembolism, which the other group was patients without stroke or thromboembolism.
Statistical analysis
Statistical analysis was performed with SPSS software (ver. 13). Results are expressed as Frequencies or percentages for categorical variables, and median (interquartile range) or mean ± SD for continuous variables. Comparisons were made by Student t-test or Mann-Whitney test for continuous variables, and Chi-square test or Fisher's exact test was used for categorical variables. P values less than 0.05 were considered statistically significant.
RESULTS
Clinical characteristics of patients
This study included 129 patients, [92 men (71.3%) and 37 women (28.7%),] with NVAF, whose average age was 63.6 +/- 11.9 years (range 34 - 86 years). Most of them (36.4%) were less than 60 years old. The median duration of follow up was 2.03 years (interquartile range 1.35 - 2.96). Among the risk factors for stroke, hypertension was most commonly noted in 75 patients (58.1%), which DM in 27 patients (20.9%). Mean time duration between 2 consecutive measurements was 29.4 +/- 10.1 days. Coronary artery disease (CAD) and heart failure (HF) were noted in 12 patients (9.3%). Because our study had reviewd the date since April 2000, the indication of OAC did not always depend on CHADS11 score. Dilated LA size (≥ 50 mm) or age ≥ 75 years was the indication of OAC. Twenty nine patients (22.5%) had CHADS2 scores of 0. Prior stroke or transient ischemic attack (TIA) before enrollment was noted only in 2 patients (1.6%) (Table 1).
INR stability
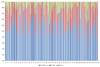
During the follow-up period, the number of prothrombin time assessment per patient was 21 ± 10. The average value of INR stability was 60.9 ± 14.9% in all the patients. The INR values which were not within INR stability were divided into two groups. One group was INR values which were below the target range (31.2%), and the other group was INR values which were above the target range (9.1%) (Fig. 1).
Factors affecting INR stability
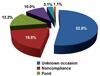
When the INR values were not within the target range, anticoagulation service asked and recorded the most appropriate reasons. It was regarded as noncompliance, when patients did not keep prescription dosage and their INR values were out of the target range. When patients told anticoagulation service that they drank an alcoholic beverage or ate something which interacts with warfarin, alcoholic beverage or something including functional foods or dietary supplements were regarded as factors affecting INR stability. Drugs or herbal remedies were similarly regarded. After finding out the reason for fluctuations of INR values, anticoagulation service spent time counselling patients and helped physicians to change dosing schedule. We did not find out the reasons affecting INR stability in significant number of cases (573 occasions: 52.8%). Of all the known factors, noncompliance was most commonly noted in 214 occasions (19.8%), food in 143 occasions (13.2%), drug in 109 occasions (10.0%), alcoholic beverage in 34 occasions (3.1%) and herbal remedy in 12 occasions (1.1%) (Fig. 2).
Comparison of INR stability between patients without and with stroke: Of 129 patients, only 4 patients had stroke during the follow-up period. The mean INR stability was 53.3 ± 4.9% in patients with stroke, and 61.2 ± 15.0% in patients without stroke. It was not statistically different between the 2 subgroups (Fig. 3).
Correlation between weekly warfarin dose and age
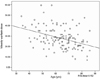
The median value of weekly warfarin dose was 27.0 (interquartile range 21.0 - 35). It seemed to be less than that of western population. It showed weakly inverse correlation with age (Fig. 4).
DISCUSSION
A significant proportion of patients with AF are not actually treated with warfarin despite its proven effectiveness in preventing stroke or systemic thromboembolism.15-17 This suboptimal use of warfarin may relate to unawareness among clinicians to guidelines and various risk stratification criteria with overestimation of bleeding risks.
It is difficult to achieve INR values within the target range in a long-term follow-up, because of fluctuations of INR values, which can be attributed to numerous factors including genetic factors, poor compliance with medication, drug to drug interactions, and change in diet.18 Furthermore, it is hard to know how long the target INR range is maintained during oral anticoagulation period. For example, even though a patient has a serial INR values in every month (for example, 1.8, 3.1, 2.7,…), it is impossible to know an accurate period which was within the target INR range; Instead, only the INR numbers which are within the target range. Therefore, we prepared a new index, INR stability, to assess the degree of optimal OAC in patients with NVAF.
Rosendaal et al.19 proposed a method to determine the time interval between 2 INR measurements, based on an assumption that actual difference in INR between any 2 consecutive measurements is linear and the data are interpolated accordingly. Days in the first half of the interval are assigned to the first INR value and days in the second half to the second INR value. Even though it does not seem to be an adequate method to determine the interval between 2 INR measurements and an annoying calculation to apply in clinical practice, there are several reports about the degree of optimal OAC in patients with AF using their method. The therapeutic range of INR was maintained how about 60% of the time in other studies.16,20 In our study, the mean value of INR stability with new method was 60.9 ± 14.9% which was similar to previous reports.
An accurate time interval within the target INR range was not calculated by the new method as well, however our method was quicker and more easily applicable assessment in clinical practice than the method of Rosendaal et al.19
The more the INR values are within the therapeutic range, the less either the ischemic stroke or bleeding complication occurs. However, our study did not show any significant differences in INR stability between patients with or without stroke. Our present study is a small population based study, and stroke incidence was very rare. Moreover, our study population included 89 patients (69%) with CHADS2 scores of 0 or 1. A large scale prospective study is needed to clarify the availability of INR stability in OAC.
The center where our study took place was a university teaching hospital. This center had anticoagulation service as well. It seemed to be a very useful system in controlling anticoagulation management, however, it exists rare by in Korea. Patients treated in other non-academic settings may not achieve this level. In other words, our study population might have a selection bias.
There was an weakly inverse correlation between weekly warfarin dose and age.
Factors which may lead to increased warfarin sensitivity are hypoalbuminemia, decreased dietary vitamin K intake, reduced absorption of vitamin K, and polypharmacy (producing drug-drug interactions that potentiate warfarin).20 These factors may be mechanisms for increased sensitivity to warfarin with aging, but further studies related with warfarin sensitivity are needed. Noncompliance was a main problem to interfere with improving INR stability. We should focus on correcting it, until warfarin is replaced with a new drug which has no interaction with drug or food, adverse effects, and need of monitoring.


 XML Download
XML Download