

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The thickness of the soft tissue in the maxillofacial area is diverse, and depends on the individual and the site. Therefore, in patients who are diagnosed or in whom the treatment protocol is designed only on the basis of tooth and skeletal measurements, errors can readily occur. In particular, in the case of orthognatic surgery for facial aesthetic improvement, accurate analysis of soft tissues should be considered a prerequisite.1 During presurgical assessment by measuring the soft and hard tissues, an aesthetic balance must be considered. For establishing appropriate treatment plans and prognosis, the estimated value of the correlation between the change in hard and soft tissues is required, and the application of such an estimated value may be of help in more accurately predicting the soft tissue lateral image after orthognatic surgery.1
Most facial deformity accompanies the protrusion or retrusion of the mentum, and therefore, surgery for the location of the mentum contributes greatly to the balance of the maxillofacial area.2 After genioplasty, the change in soft tissues is diverse, depending on the individual and the presence or absence of other simultaneous surgery.3
The purpose of this study was to measure the anteroinferior changes and the degree of vertical changes to facilitate the prediction of treatment outcome in patients undergoing genioplasty only, genioplasty with bilateral sagittal split ramus osteotomy (BSSRO), genioplasty, or BSSRO and Lefort I osteotomy.
MATERIALS AND METHODS
Patients
This study was carried out on 25 patients who underwent genioplasty at the Department of Oral and Maxillofacial Surgery at Chosun University Dental Hospital, Korea, from January 2001 to December 2007, and who were available for follow-up. Twelve male and thirteen female patients (mean age 22.3 years; range 17-37) participated.
Methods
In patients undergoing genioplasty only, genioplasty with BSSRO, or genioplasty with BSSRO and Lefort I osteotomy, cephalometric radiographs were taken prior to surgery, and after 1 week and 6 months of the surgery. Perspective maps were prepared. Subsequently, using the V-ceph program, the relative changes in the vertical and anteroposterior directions were compared and analyzed (Figs. 1-3).
The measurement sites of hard and soft tissues were nasion (N), sella (S), menton (Me), pogonion (Pog), B point (B), soft tissue nasion (Ns), labialis inferius (Li), soft tissue B point (Bs), soft tissue pogonion (Pogs), and soft tissue menton (Mes). The baseline was defined as the horizontal plane (HP) of the line connecting the N and S moved by 7° in the clockwise direction, based on S. This line was chosen because the angle formed by the Frankfurt horizontal (FH) plane close to the physiological horizon with the sella-nasion (SN) plane is 6-7°, and the SN plane has a relatively good reproducibility and reliability. Past the hard tissue in the menton, past the line parallel to the HP, past the soft tissue in the menton, and based on the line parallel to the HP, we measured the vertical distance between the HP and two lines of a line vertical to the HP and a line drawn based on S, and by measuring the transverse line to the hard tissue B point, Pog, soft tissue Li, Bs, and Pogs, and we calculated the amount of vertical and transverse change (Fig. 4).
Operation
Incision was made through the mucosa of the lower lip, nonetheless, the method extending to the utmost lateral side of the buccal vestibule is of help in accessing the bone exposure and the mental nerve. The incision was extended to both premolar teeth, and periosteum was dissected. The mental nerve was assessed, and the lower border of the mandible was exposed after inferior and anterior dissection. Using a reciprocating saw, transverse osteotomy was performed in the inferior B point. Additional myotomy of the digastric or mylohyoid muscle was not performed, and it was fixed with a chin plate and a titanium miniplate after moving the mentum.
RESULTS
Eight male and nine female patients underwent genioplasty with BSSRO, and four male and three female patients underwent genioplasty with BSSRO and Lefort I osteotomy. Only one female patient underwent genioplasty only (Table 1). Advanced genioplasty with a mean of 4.8 mm was performed in 17 patients, and setback genioplasty with a mean of 3.3 mm in 8 patients (Table 2).
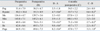
Regarding statistical significance at the 95% reliability, SPSS (SPSS Inc., Chicago, IL, USA), Pog, B point, Li, Bs, and Pogs were significant, the mean regression level of B point was 13.0%, the mean regression level of Bs was 23.1%, and the mean regression level of Pogs was 39.8%, which was found to be slightly high. The mean amount of change in Pogs, Bs, and soft tissue Li against Pog and B point was 0.9 (Table 3).
DISCUSSION
The motives for patients undergoing genioplasty are very diverse and complex. Major factors are compensation of functional defect, as well as social and psychological reasons; however, the most important primary reason is aesthetic.4 Various genioplastic surgical methods have been used to treat patients with maxillofacial deformity. Patients planning to have genioplasty go through surgery with the expectation of improvements in functional, social, and psychological aspects. Aesthetic changes vary depending on the amount of change in hard tissues, and computer programs predicting the maxillofacial change after surgery have recently provided numerous incentives to patients.4 Therefore, the purpose of genioplasty is to correct abnormal functions such as mastication and pronunciation, and to achieve superior aesthetic results and stability after surgery. To predict the change in the maxillofacial profile while planning the treatment, the predicted change in facial soft tissues is an important reference while performing surgery.
Previous methods had almost no conception of functional aspects, and that hard tissues must be balanced with soft tissues in the mental area, including adjacent muscles. Regarding the surgical techniques themselves, shortcomings included difficulty in achieving accurate replacement of distal fragments, stability, and fixation during surgery.5
Ayoub, et al.6 reported that changes in soft tissues are complex, rather than a 1 : 1 relationship with skeletal change, and that they are influenced by the interaction of diverse variables, including the skeleton, dental changes, lip tension, soft tissue thickness, and muscle function. Fanibunda7 demonstrated that the final location of soft tissues after orthognatic surgery is determined by the three-dimensional interrelationship of hard and soft tissues prior to surgery. For the final prediction of facial aesthetics, the degree of overbite or overjet, the presence or absence of cleft lip closure, muscles prior to surgery, subcutaneous tissues, and the elasticity of the skin have to be considered.
Busquets8 reported that in a retrognathic patient, the amount of change in Pog was 0.8 : 1 against the FH plane and 0.4 : 1 against Li. Scheideman, et al.9 stated that in six cases treated with mandibular setback and advancement genioplasty, the amount of the change in Pog was 0.87 : 1. In addition, McDonell, et al.10 reported that in 15 cases, after undergoing advancement genioplasty, the rate of the change in Pog in soft and hard tissues was 0.75 : 1.
Among bone fragment fixation methods, those that move a bone fragment to a desired site and put it in position involve mainly intermaxillary fixation using stainless steel wires or a miniplate. Both methods of fixation are effective, although the miniplate method is more reliable, easy to apply, and has been used more widely. With stainless steel fixation using a miniplate, the muscle layer is relatively thick, and in the mental area where blood supply is abundant, little possibility of developing postsurgical complications, such as palpation of the metal plate and infection, exist. However, complaints of patients for secondary genioplasty, removal of the miniplate, or bone growth on the upper side of the miniplate result in the miniplate being buried. Stainless steel fixation using a miniplate may help bone healing by more definite fixation of the displaced bone fragments; nonetheless, in areas where the bone is reformed continuously after surgery, the long-term prognosis of the metal plate is uncertain.4
Among surgical techniques, soft tissue treatment may influence stability and regression after surgery. Bell and Gallagher11 and Wolford and Bates12 reported that in soft tissue treatment, the thickness of soft tissue decreases when the anterior and posterior peristeum is peeled away completely.
In the analysis of cephalometric radiographs, by getting a standardized measurement prior to surgery and after surgery, and defining the measurement sites, the procedures will be reproducible, thus minimizing measurement errors. Therefore, the establishment of a surgery plan considering postsurgical stability through long-term follow-ups may be required. In addition, standards are required to subclassify the effects of surgical and fixation methods and other factors. Studies using more patients may be needed to improve the measurement of statistical significance.
This study was performed on 25 patients, who were available for follow-up, recruited from those undergoing genioplasty at the Department of Oral and Maxillofacial Surgery at the Chosun University Dental Hospital from January 2001 to December 2007. Cephalometric radiographs were taken prior to surgery, and in a week and 6 months of surgery. Pog, B point, Me, Pogs, Bs, Li and Mes were measured, and the following conclusions were obtained: The average regression level of B point was 13.0% and the average regression level of Pogs was 39.8%; the vertical regression level was not significant; the average amount of change in Pogs, Bs, and Li versus Pog and B point was 0.86; and the average amount of change in Mes against Me was 0.66.






 XML Download
XML Download