

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Attention deficit hyperactivity disorder (ADHD) is a clinical disorder characterized by persistent hyperactivity, inattention, and impulsivity.1 Symptoms appear to be developmentally inappropriate and lead to functional impairments at home or in school.2 Children with ADHD are more likely to have comorbid learning difficulties and behavioral problems, and to have poor peer relationships and low self-esteem.3 About 30-50% of children with ADHD have significant behavior and psychiatric problems in adulthood.4-6 Persistence of ADHD symptoms into adolescence and adulthood is associated with antisocial behavior, substance use and abuse,7 fewer years of education, and lower rates of employment.8
Symptom control is strongly related to functional improvement.9-11 Methylphenidate (MPH) is recommended for the treatment of ADHD.12 Studies indicate that MPH is an effective remedy for both core symptoms (e.g., inattention, hyperactivity, and impulsivity) and aggressive behavior.13 MPH increases child compliance with parental commands and decreases hostile and negative responses, which facilitates the social interactions in young children.14-16 However, about 30% of children with ADHD do not tolerate or respond to stimulant medication.17,18 A study reported that the electroencephalogram (EEG) patterns of children who respond to MPH treatment are different from those who do not respond.19 However, little else is known regarding predictive factors for responsiveness to MPH. Further research into these predictive factors is warranted.
Studies have consistently shown that great response time (RT) variability is found in children with ADHD, making it a potential marker for differentiating children with ADHD from those without ADHD.20-26 Homozygosity for the DAT 10-repeat allele is correlated with poor response to MPH treatment among Korean children with ADHD.27 Furthermore, ADHD patients who have two copies of the 10-repeat allele at the dopamine transporter gene (DAT) show greater variability in RT on attention tests compared to those with fewer than two copies.28 These data suggest the possible relationship between greater RT and poor response to MPH treatment. We performed this study to examine whether great RT variability would be predictive of poor response to MPH treatment in children with ADHD.
MATERIALS AND METHODS
Participants
Participants were recruited from seven sites in Korea for a prospective 12-week, open-labeled study to examine optimal dosage of OROS methylphenidate. Diagnoses were made with the Kiddie-Schedule for Affective Disorders and Schizophrenia-Present and Lifetime Version (K-SADS-PL).29 Exclusion criteria were as follows: use of MPH hydrochloride other than OROS-MPH within the past 24 hours; use of OROS-MPH within the past three months; use of psychotropic medication within the past four months (clonidine or other α-adrenaline agonist, tricyclic antidepressant, selective serotonin reuptake inhibitor, theophylline, coumarin, or anticonvulsant, antipsychotics, benzodiazepine, modafinil); history of hypersensitivity reaction to MPH hydrochloride or another component of OROS MPH; other medical problems, such as gastrointestinal disorders, glaucoma, cardiovascular disease, or hyperthyroidism; neurological illnesses, such as a seizure disorder; comorbid psychiatric disorders, such as pervasive development disorder, psychotic disorder, or Tourette syndrome; an intelligence quotient (IQ) less than 70 [as assessed by the Korean Wechsler Intelligence Scale for Children (K-WISC-III)30]; history of substance use or abuse; and possible pregnancy. After an initial assessment, 144 subjects (ages 6-18 years) with ADHD were included.
Baseline MPH dosages were either 18 mg or 27 mg depending on clinical judgment. Dosage was titrated for nine weeks, at which point it was maintained for the remainder of the 12-week treatment trial. Of the 144 subjects enrolled in the study, 28 dropped out due to adverse events (n = 8, 28.6%), medication noncompliance (n = 12, 42.9%), or follow-up loss (n = 6, 21.4%). Data from an additional 24 subjects with comorbid disorders, such as oppositional defiant disorder (n = 12), tic disorder (n = 9), depressive disorder (n = 3), and anxiety disorder (n = 6), were excluded. Since the ADHD diagnostics system was standardized for children of 6-15 years, we excluded 2 subjects who were older than 15. Thus, data from 88 participants were included in the final statistical analyses.
This study was approved by the Institutional Review Boards of all seven sites.
Measures
Symptom severity and treatment effectiveness
The attention deficit hyperactivity disorder rating scale (ARS; Korean version, K-ARS) is an 18-item measure used to assess inattention and hyperactivity. Items are rated on a 4-point scale (0 = never or rarely, 3 = very often). The K-ARS has good reliability and validity among Korean children.31 The IOWA Conners Parent Rating Scale (CPRS) is a 10-item measure administered to parents to assess inattention/overactivity (5 items) and oppositional/defiant behavior (5 items) in children.32 The CPRS has a 4-point rating scale (0 = never, 3 = very often) and it has good reliability and validity.32 The Clinical Global Impression Severity (CGI-S) and Clinical Global Impression Improvement (CGI-I) scales are clinical outcome measures. Both are clinician-administered and consist of 7-point scales (1 = much improved, 7 = much worse). Generally, the CGI-I is more sensitive to treatment effect.33 We defined 'responders' as subjects who received a score of less than 18 on the K-ARS and a score of 1 or 2 on the CGI-I, and ultimately were in remission state.34 Clinical assessment was done at baseline as well as weeks 1, 3, 6, 9, and 12. Body weights and vital signs were measured at every visit. ECG and laboratory measures were assessed at baseline and week 12.
ADHD diagnostic system
The ADHD diagnostic system (ADS) is a computerized continuous performance test that consists of auditory and visual modalities.35 In each modality, the targets and non-targets are presented in the form of auditory or visual stimuli. The test can be used to assess children over five years of age. It consists of three sessions: the early, middle, and late phases. The ADS generates four broadband scores. The omission errors score indicates the number of times when the subject failed to respond to the target, with high scores reflecting inattention. The commission errors score indicates the number of times when the subject made an incorrect response to the non-target, with high scores reflecting impulsivity. The response time (RT) score measures the amount of time between presentation of the target stimulus and a correct response. RT is related to speed of information processing and motor response. The standard deviation of the RT reflects variability or consistency of attention.35 Scores are reported as T-scores and produced in a printable report. In our study, each subject performed the ADS at baseline and at the end of the study. We used scores derived from the visual modality of the ADS in light of research suggesting that the auditory modality is more difficult than the visual modality and is less sensitive in differentiating subjects with ADHD from healthy controls.35
Statistical analyses
To examine the effect of the RT variability on the MPH treatment response, we carried out analysis in two phases. At the first phase, we conducted T-tests, chi-square tests, Mann-Whitney U tests and univariate analysis of variance (ANOVA) to determine whether the responders differed significantly from the non-responders on the focal variables and extract the predictor variables. The RT variability was entered as an independent variable and commission error score was entered as a covariate for univariate ANOVA. Secondly, to examine the effect of the baseline RT variability on the MPH response, we conducted a binary logistic regression analysis, with baseline RT variability entered as the predictor variable, and "responder/non-responder" as the dependent variable. We ran a series of paired T-tests to compare the baseline and 12 week ADS scores. We then computed correlations to examine the relationship between the ADS scores and the behavior rating scale scores.
RESULTS
The mean age of the participants at baseline was 9.43 years (± 2.2). Slightly more than 87.5% (n = 77) of the children were boys and 11 (12.5%) were girls. The average IQ was 109.7 (± 16.1). The mean K-ARS and CPRS scores were 28.2 (± 8.5) and 11.7 (± 5.3), respectively.
Characteristics of the responders (n = 59) and non-responders (n = 29) are shown in Table 1. There were no significant differences between the responders and non-responders for age or gender. Nor were there any significant differences between the responders and non-responders for baseline IQ, K-ARS, and CPRS scores.
At week 12, the mean dosage of MPH across subjects was 0.99 mg/kg (± 0.29). There was no statistically significant difference in week 12 MPH dosage between the responders and non-responders. At week 12, the responders scored significantly lower on the K-ARS and CPRS compared to the non-responders (Table 1).
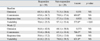
The ADS scores are summarized in Table 2. At baseline, the result of univariate ANOVA showed that the non-responders had significantly greater RT variability compared to the responders (F = 5.330, p = 0.028). However, there was no significant difference in commission error between responders and non-responders. The non-responder RT variability at week 12 was 78.0 (± 39.5), which is out of normal range and has clinical significance.35
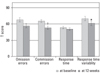
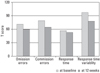
There was a significant decrease in commission errors and RT variability from baseline to week 12 among the responders (Fig. 1). The means of all four scores fell within the normal range. Similarly, there was a significant decrease in commission errors and RT variability from baseline to week 12 among the non-responders (Fig. 2). However, among the non-responders, RT variability was greater than 70 even after 12 weeks of treatment.
The ADS scores were not correlated with the K-ARS and CPRS scores at baseline or at week 12.
RT variability at baseline was a significant predictor of treatment response at week 12 (Nagelkerke R2 = 0.136, p < 0.01). It predicted 94.9% of responder, 17.2% of non-responder and 69.3% of overall group.
DISCUSSION
In the present study, the non-responders showed greater RT variability at baseline. Great RT variability may reflect dysfunctional prefrontal activity and inefficient top-down control of attention.36 In a longitudinal study to evaluate the neuropsychological functions of children with ADHD, Halperin, et al.37 reported that a deficiency in response variability remained at the 10-year follow-up regardless of remission status. Great RT variability seems to indicate high risk in terms of the persistence of deficit in ADHD. Our results together, with those of earlier studies20,37 suggest that patients with great RT variability may have more severe neuronal dysfunction and high RT may indicate poor outcome.
We found no significant correlations between RT variability and the K-ARS and CPRS scores, which is in line with previous study, indicating that scores on continuous performance tests have low correlations with ADHD clinical symptom severity.38 In spite of the significant difference in baseline RT variability between the responders and non-responders, there was no significant difference in baseline clinical symptom severity between the responders and non-responders. This suggests that MPH treatment responsiveness is independent of baseline clinical symptom severity. Furthermore, regardless of the responsiveness to treatment, we found significant decreases in commission and RT variability after treatment. This also supports previous finding to show low correlation between clinical symptoms and CPT test results.
It is generally accepted that MPH can decrease the errors of omission.39 In the present study, there was a tendency to decrease in the errors of omission after treatment, however it did not reach statistical significance. Small sample size would be a possible explanation.
To our best knowledge, we are the first to present findings to indicate that great RT variability may predict poor response to MPH treatment. Although Coghill, et al.40 examined whether baseline neuropsychological functioning predicted clinical response to MPH, they did not include a measure of RT, therefore, their results could not be compared to ours.
This study has several limitations that should be noted. First, a placebo control group was not included in the study design. Second, we did not perform a time series analysis. Since ADS program only preserves summary data and converts T scores after completion of the task, we were unable to collect response time from each response. Studies using time series analyses of RT data suggest that RT variability can be broken down into heterogeneous components.21,25 In a time series analysis of data gathered from a Sustained Attention to Response Task (SART), Johnson, et al.41 reported that RT variability has 'fast' and 'slow' components, and that the fast component of RT variability reflects moment-to-moment variability and is predictive of response to MPH treatment, whereas the slow component of RT variability reflects a gradual deterioration in RT variability and is not predictive of response to MPH treatment. They also found no significant difference between the subjects with ADHD and the healthy controls in slow variability RT, suggesting that this component of RT may not tap into the deficits associated with ADHD. We were unable to compare our findings with those of Johnson, et al., as we used a different measure of RT variability, but future research to determine the predictive powers of the fast and slow components of RT variability is needed using a time series analysis. Third, the worst responders might have been dropped out due to lack of compliance. The effect was still found, nevertheless, the effect seen in this study might be underestimated.
In spite of these limitations, the present study has implications for clinical work. Our finding to suggest that RT variability may be predictive of MPH treatment response provides clinicians with a possible clinical indicator to be used in treatment planning with MPH.

 XML Download
XML Download