

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Facet tropism is defined as asymmetry in both the facet joint angles of the lumbar and lumbosacral regions.1-7 For many years, the effect of facet tropism on the development of intervertebral disc degeneration has been debated.1-8 However, the specific details regarding the effects of facet tropism on the development of degenerative disc disease remains as the subject of debate. Most of the previous facet tropism studies have focused on the relationship between facet tropism and lumbar disc herniation.1,4-10
The role of facet tropism in the pathogenesis of lumbar degenerative disc disease is not fully understood Currently, controversy exists surrounding the question of whether or not any significant relationship exists between facet tropism and the development of disc or facet joint degeneration.1-3,11 Additionally, the relationship between facet tropism and degenerative spondylolisthesis and translational segmental motion is highly controversial.1-3,11
In the current study, we attempted to evaluate the effect of facet tropism on disc and facet joint degeneration. Additionally, the relationship between facet tropism and changes in translational segmental motion was investigated.
MATERIALS AND METHODS
Population
This study consisted of 300 patients, aged 18-80 years (average age, 41.2 years). These individuals were selected from a larger population of patients with low back pain or sciatica. Patients with severe scoliosis, spina bifida, transitional vertebra, spinal infection, spondylolysis, and/or malignant spine tumors were excluded.
KMRI measurement and grading
MR imaging of the lumbar spine was performed using a 0.6 Tesla MRI scanner (Fonar Corp. Upright, Multi-Position™, New York, NY, USA). Images were obtained using a quad channel planar coil. An 18-inch gap between the magnets is present. T1-weighted sagittal spin echo images (repetition time 671 ms, echo time 17 ms, thickness 4.0 mm, field of view 30 cm, matrix 256×224, NEX 2) and T2-wighted fast spin echo images (repetition time 3,000 ms, echo time 140 ms, thickness 4.0 mm, field of view 30 cm, matrix 256×224, NEX 2, flip angle) were obtained.
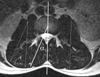
Using axial images, the facet joint angle for each facet joint corresponding to 900 functional spinal units at L3-L4, L4-L5, and L5-S1 were measured. Facet joint angles were measured based on Noren, et al.'s method.12 T-2 axial images that equally bisected the intervetebral disc space were used to measure each facet angle. The facet angle corresponds to the angle between the reference line that passes through the center of the disc and the base of the spinous process and the facet line that connects the anteromedial and posterolateral margins of the superior articular facet (Fig. 1).
The mean and standard deviation (SD) of the tropism angles were calculated. From this calculation, each pair of facet joints was classified as symmetric (within 1 SD of the mean), or asymmetric (beyond 1 SD of the mean).19 For this study, facet tropism or facet asymmetry was defined as a bilateral angle difference greater than 7° which corresponded to 1 SD. According to the presence/absence of facet asymmetry, discs at each level were classified into two groups. Discs with facet asymmetry between both sides greater than 7° were placed in the facet tropism group, while discs with a facet angle difference less than 7° between both sides were placed in the facet symmetry group. The facet tropism group had 97, 108, and 109 segments at L3-L4, L4-L5, and L5-S1, respectively. Age and gender were not found to have any significant correlations with either group (Table 1 and 2).
Intervertebral disc degeneration was evaluated using T2-weighted sagittal KMRI. Disc degeneration was classified into five grades according to Pfirrmann's classification system.13 Grade I corresponded to normal discs and Grade V corresponded to discs with advanced degeneration. Facet joint degeneration was graded based on the four grades used by Fujiwara et al.14 Grade 1 corresponded to normal facet joints, and grades 2, 3, and 4, corresponded to mild, moderate, and severely degenerated facet joints, respectively.
Translational segmental motion was measured using observed KMRI from flexion to extension positions. Translational segmental motion was calculated using the absolute value of the difference between vertebral body location during flexion and extension (Fig. 2). All calculations were acquired using MR Analyzer software (TrueMRI Corporation, Bellflower, CA, USA).
Statistical analysis
The incidence of facet tropism according to age and gender was analyzed using the Student t-test and X2 test. The relationship between facet tropism and disc and facet joint degeneration was examined using the X2 test. Statistical analysis of the relationship between facet tropism and translational segmental motion was performed using the student t-test. For all computations, statistical significance corresponded to p < 0.05.
RESULTS
The incidence of facet tropism was 34.5% at L3-L4, 35.2% at L4-L5 and 35.2% at L5-S1. The mean facet joint angle was 35° at L3-L4, 39° at L4-L5, and 48° at L5-S1. The mean facet joint angles at each level were significantly different from one-another (p < 0.05).
Disc degeneration
No significant correlation between facet tropism and disc degeneration was observed (Table 3). The facet tropism group had a greater number of highly degenerated discs than the facet symmetry group at L4-L5. However, this difference was not statistically significant.
Facet joint degeneration
Facet tropism was found to be associated significantly with facet joint degeneration at L4-L5.The incidence of high grades of facet joint degeneration at L4-L5 within the facet tropism group was significantly higher than in the facet symmetry group (p < 0.01) (Table 4). However, at L3-L4 and L5-S1, no significant association between facet tropism and facet joint degeneration was found.
Translational segmental motion
At all levels, the values of mean translational segmental motion of facet tropism group were higher than those of facet symmetry group. However, a correlation was observed between facet tropism and translational segmental motion at L3-L4, L4-L5, and L5-S1 was not significant (Table 5).
DISCUSSION
Facet tropism is defined as asymmetry between the left and right facet joint angles of the lumbar spine. Asymmetry in the orientation of the zygapophyseal joint surfaces is not uncommon, with estimates of its occurrence at 10-70.5% of the population.3-5 Our study revealed an incidence of facet tropism in 35% of the spinal units which were taken into consideration. Facet tropism is most common at L5-S1, followed by L4-L5.15
The criteria for determining facet tropism have varied greatly, although the actual definition of facet tropism is asymmetry between the right and left facet joints. In the lumbar spine, the majority of facet joints vary by less than 7° in orientation between the two sides.3 Noren et al.12 defined facet asymmetry as a bilateral angle difference greater than 5°. In other biomechanical studies, facet asymmetry was defined as a difference in facet angles greater than 1-10° or one SD.4,5,16 Grogan, et al.3 divided facet joint tropism into three distinct classifications. When the orientation differed from one side to another by more than 7°, the facet joints at that level were defined as having tropism.1 Moderate tropism was defined as a difference of 7° to 15° between the orientation of the joints (one SD from the mean difference) and severe tropism was defined as a difference of more than 15° (two SDs from the mean) between the two sides. For the current study, the authors defined facet tropism to be bilateral angular asymmetry greater than 7°.
The angular difference inherent to facet joint tropism causes biomechanical issues. By definition, facet joint degeneration exists when one joint has more coronal orientation than the other. Farfan and Sullivan17 emphasized the importance of coronally facing facet joints upon the development of lumbar disc herniations. Coronally facing facet joints offer little resistance to shear intervertebral force, so that the joints tend to rotate toward the side of the more coronary facing facet joint, possibly leading to additional rotational stress on the annulus fibrosus.16 Loback, et al.18 showed that facet joint asymmetry is found more likely on the side of the coronally facing facet joint. When tropism was present, the motion segment was found to have a tendency to rotate towards the more oblique joint when axial loads were applied.16 This asymmetric axial rotation caused by tropism can place additional torsional loads on the intervertebral discs which can lead to intervertebral disc injury and degeneration. This biomechanical mechanism was used to describe the development of lumbar disc herniation, disc degeneration, and degenerative spondylolisthesis associated with facet tropism. Some studies have claimed that lumbar facet joint tropism does not accelerate degeneration of the facet joints.1,3 For the current study, the authors chose to investigate facet tropism and some of the findings associated with lumbar degenerative disc disease, including disc degeneration, facet joint degeneration, and spondylolisthesis (translational segmental motion).
The role of facet tropism in the pathogenesis of disc degeneration is a contested issue. Boden, et al.1 and Vanharanta, et al.19 reported no significant correlation between facet tropism and disc degeneration. However, Noren, et al.12 concluded that the existence of facet tropism can increase the risk of disc degeneration. Additionally, Dai2 reported that a significant correlation existed between facet joint tropism and the degree of disc degeneration in patients with degenerative spondylolisthesis. In the present study, no significant correlation was observed between facet joint tropism and disc degeneration at L3-L4, L4-L5, or L5-S1. However, a higher (but not statistically significant) incidence of highly degenerated discs at L4-L5 was observed within the facet tropism group.
Grogan, et al.3 concluded that lumbar facet joint tropism does not accelerate facet joint degeneration. They reported no significant differences in facet joint degeneration between facet joints with and without tropism.3 However, there are many limitations associated with this study. It was based on a small number of specimens (21 cadavers) and an even smaller number of lumbar facet joints exhibiting facet tropism (10 out of 104 lumbar facet joints). Additionally, this study did not take the level, where the tropism occurred, into consideration. Our current study included L3-L4, L4-L5, and L5-S1 facet joints belonging to 300 living participants and our findings were found to be similar to Grogan et al.'s at L3-L4 and L5-S1. However, at L4-L5, a significant correlation between facet joint tropism and facet joint degeneration was observed. Based on the fact1,4 that L4-L5 experiences the most segmental flexion and extension within the lower lumbar spine, this result suggests that the existence of facet tropism within highly mobile lumbar segments could affect the development of facet joint degeneration.
Berlemann, et al.11 reported that facet joint asymmetry does not seem to play a major role in the development of degenerative spondylolisthesis. However, Dai2 found that facet joint tropism was a predisposing factor for the development of degenerative spondylolisthesis. The present study found no association between facet tropism and translational segmental motion (such as vertebral slippage) within the lumbar spine. Our results indicate that facet tropism has no major association with the development of degenerative spondylolisthesis.
Previous reports have shown that facet orientation has a significant association with degenerative spondylolisthesis.1,2,11 Additionally, some of these studies reported that, in patients with degenerative spondylolisthesis, the transverse plane of facet joints was more sagittally oriented.2,11 All of these studies found that individuals with larger facetjoint angles, relative to the coronal plane (more sagittal orientation of facet joint), exhibited a higher incidence of degenerative spondylolisthesis. Although facet orientation was not taken into consideration for this study, the authors believe that it is an important element for understanding all of the factors that lead to the development of spondylolisthesis, and that this topic should be investigated further.
Another interesting factor to take into consideration is the existence of facet joint tropism within normal spines. This raises questions as to the root causality of facet joint tropism. Facet joint tropism could be caused by an inborn characteristic of the human spine, as a result of mechanical stresses on the spine (i.e., asymmetric loading of the human spine) or as a consequence of existing spinal deformities (i.e., scoliosis).20 Noren, et al.12 documented that subjects with lumbar degenerative disc disease had a higher incidence of facet joint tropism than the normal population. The nature of the relationship between facet joint tropism and degenerative changes within the lumbar spine remains a controversial topic. Essentially, there are two sides to this debate, one advocating that facet tropism leads to degeneration2 and the other claiming that certain degenerative statuses (i.e., degenerative spondylolisthesis) lead to facet tropism.1,11 Our results show that, at active functional spine units, facet tropism partially influences the development of facet joint degeneration. This seems to give legitimacy to the theory that facet tropism can lead to facet joint degeneration, although further investigation into the relationship between facet tropism and facet joint degeneration is necessary.
Our study has several limitations. First, this was a cross-sectional observational study on facet angle. Second, our study was limited by geometrical considerations. Even if facet joints often were not planar, our measurements did not take into account the complex three-dimensional geometry of the facet joints and their relationship with the disc and facet joint degeneration. Due to these limitations, further study is needed in the future.
The data presented in this study suggests that facet tropism is correlated significantly with facet joint degeneration in segments which are involved in frequent segmental motion. However, no significant relationship was observed between facet tropism and the development of disc degeneration or degenerative spondylolisthesis.





 XML Download
XML Download