

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cholesterol granuloma (CG) of the middle ear typically presents as a conductive hearing loss and a blue eardrum, whereas those at the petrous apex either manifest as the side effects of bony erosion (with sensorineural hearing loss, tinnitus, vertigo, or cranial nerve impairment), or are incidentally identified.1 CG can be a perfectly localized and isolated mass in any pneumatized area in temporal bone, the middle ear cavity,2,3 mastoid antrum,4 external auditory canal,5 or the petrous apex,1 as has been found in as many as 12 - 20% of temporal bones with chronic otitis media.2-4 According to a histopathologic study, CG may be present in 12% of patients with chronic otitis media with an intact tympanic membranes, and in 21% of those with a perforated tympanic membrane.6 However, intramembranous tympanic membrane CG occurs less frequently, and only one case has so far been reported in the English literature.7 Here, we report our experiences with a case of CG in the tympanic membrane and review relevant medical literature.
CASE REPORT
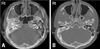
A 42-year-old man presented with a history of childhood coalescent otitis media and, as consequent, hearing loss in the right ear. He complained of middle ear fullness without otalgia. A blue eardrum was identified at the local clinic. The patient was referred to our department. Otomicroscopic findings of the right tympanic membrane demonstrated a bulging blue eardrum. Two weeks after presentation, otomicroscopic findings showed a pinhole perforation in the anterior area with a brown discharge. A pure tone audiogram showed a dead ear on the right side (Fig. 1). High resolution temporal bone CT showed a bulging mass shadow in the middle ear and a dense soft tissue lesion, which filled both the epitympanum and mastoid cavity. New bone formation was noted between the epitympanum and middle ear (Fig. 2A), and bulging soft tissue in the middle ear (Fig. 2B). No definite ossicular shadow was identified. Tympanomastoidectomy was performed under general anesthesia, and new bone formation was confirmed in the mastoid antrum and epitympanum, the latter of which was blocked by the new bone. No ossicular structure was identified in the epitympanum. The dead ear finding is believed to have been caused by a complication of childhood coalescent otitis media. After elevation of the tympanomeatal flap, the tympanic membrane revealed a round, brownish mass with a glistening surface and a severely thickened pars tensa (Fig. 3). The incus and stapes were not identified. After removing the mass from the tympanic membrane, it was sent for pathological examination, which confirmed CG (Fig. 4). Postoperatively, the patient had an uneventful course without any sign of blue eardrum recurrence.
DISCUSSION
Three factors are considered to play an important role in the development of CGs: interference with drainage, hemorrhage, and ventilation obstruction,8 although remaining mesenchyme9 and hematopoietic bone marrow10,11 have also been suggested to be associated with CG formation.
Clinically, CG of the temporal bone appears in three forms:12 in association with chronic otitis media (especially cholesteatoma), idiopathic hemotympanum, or a localized lesion in the middle ear, mastoid antrum, external auditory canal, and petrous apex. CG can also occur without any previous history of infection.2,13
In the present case, the patient had a history of otitis media from childhood. Moreover, the bulging tympanic membrane had a pinhole perforation with brown discharge in the anterior pars tensa. CGs contain hemosiderin, lipids, and cholesterol crystals. Microscopically, these crystals are surrounded by foreign body giant cells in fibrous connective tissue, which is infiltrated by round cells.2
Jaisinghani et al.14 correlated pathologic findings of the tympanic membrane with pathologic changes in the middle ear cleft in cases with chronic otitis media in 150 temporal bones. They found a significant correlation between CG and tympanic membrane retraction and a mild additive effect when retraction was associated with perforation, however, the described case showed no tympanic membrane retraction. CG in the tympanic membrane has been rarely reported. In a recently published case, Haginomori et al.7 reported histopathological characteristics of CG in the tympanic membrane, and speculated that, when hemorrhage occurs in the tympanic membrane, it is likely due to the absence of drainage or air exchange systems. On the other hand, when a CG develops in the tympanic membrane, it may promote its own growth in a vicious circle, by becoming another source of hemorrhage from small vessels whose numbers continue to increase.
Park15 suggested that blue eardrum is an independent clinical entity, and found no bone changes with temporal bone CT or surgical findings. In the present case, however, temporal bone CT showed new bone formation in the epitympanum. Moreover, intraoperative findings indicated a complete attic block by new bone formation.
This finding together with the resolution of blue eardrum indicate that the main reason for blue eardrum in the present case was CG at the tympanic membrane.
In conclusion, we report a case of CG of the tympanic membrane, which presented as blue eardrum.



 XML Download
XML Download