

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Seminal vesicle cyst is an extremely rare disease, occurring in 0.005% of the population.1 It is often associated with other anomalies. Especially, Zinner2 reported a seminal vesicle cyst in combination with ipsilateral renal agenesis in 1914, and the associated anomaly has been reported in literatures.3-5 Treatment of the seminal vesicle cyst can be decided according to symptom existence. When surgical treatment for symptomatic seminal vesicle cyst is deemed necessary, conventional surgery is frankly invasive because of the deep location and dissection difficulty of the seminal vesicles in the retrovesical space. Recently, the laparoscopic approach has been advocated as an optimal minimally invasive technique for the surgical treatment of seminal vesicle pathology. It provides a good image and easy approach for the seminal vesicle.6,7
We present 4 cases of seminal vesicle cyst with ipsilateral renal agenesis, which were successfully treated by laparoscopy.
MATERIALS AND METHODS
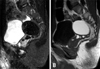
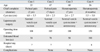
From May 2003 to January 2008, 4 patients with seminal vesicle cysts with ipsilateral renal agenesis were presented at our hospital. The mean age was 45.8 years (22 - 68). Chief complaints were perineal pain in two patients and hematospermia in two patients. Diagnostic procedures included digital rectal examination, transrectal ultrasonography (TRUS), abdominopelvic computed tomography (CT), pelvic magnetic resonance imaging (MRI), and cystoscopy. TRUS showed cystic masses with heterogenous contents adjacent to the left seminal vesicle in all cases. Cyst sizes were 6.0×5.5 cm, 3.0×2.5 cm, 2.6×2.7 cm, and 5.5×5.0 cm (Table 1). Pelvic MRI also showed round cystic masses in the left seminal vesicles with contents of high signal intensity in T1 weighted image and low signal intensity in T2 weighted image (Fig. 1). Abdominal CT scan revealed no left kidney and remnant ureter in the retroperitoneal space. The remnant ureter inserted into the seminal vesicle cyst (Fig. 2). Cystoscopy revealed hemitrigones with no left ureteral orifices in all cases.
Seminal vesicle cysts and remnant ureters were excised by laparoscopic surgery under general anesthesia. Firstly, in a lithotomy position, the verumontanum and ejaculatory duct were observed with a 7 / 13.5F ureteroscope. Under the ureteroscopic guidance, a 0.035-inch guide wire was inserted into the seminal vesicle cyst and remnant ureter. A Foley catheter was placed into the bladder.
The patient was positioned in a supine position for a laparoscopic surgery. A transperitoneal access is achieved with Veress needle. Four ports were used, a 5/12-mm trocar at umbilicus, a 5/11-mm trocar at the right lateral border of the rectus muscle at the 5 cm lower level of the umbilicus, a 5/11-mm trocar at the left lateral border of the rectus muscle at the 5 cm lower level of the umbilicus, and a 5-mm trocar at the left lateral border of the rectus muscle at the 5 cm above level of the umbilicus.
Once the descending colon was mobilized medially, the left ureter was detected in the retroperitoneal space. It was dissected cephalad above the iliac vessel. There was no renal tissue in the end of the ureter. The lower ureter was dissected to the bladder. The bladder was retracted anterior. A junction of the ureter and seminal vesicle was seen (Fig. 3). The guide wire was detected in the communicated area. The seminal vesicle was dissected and sectioned with ultrasonic scissors and clips. The whole specimen was removed through the umbilical port.
RESULTS
The mean operative time was 133.8 minutes (range, 100 - 180). The mean hospital stay was 6.8 days (range, 5 - 8). There were no operative complications and transfusions. The mean estimated blood loss was 85 mL (range, 30 - 190) (Table 1). In all patients, oral intake and ambulation were resumed on postoperative day 1. The urethral Foley catheter was removed on postoperative day 1.
The pathological assessments of the specimens revealed benign seminal vesicle cyst in all cases. The cystic walls were composed of fibrous connective tissue. They were lined by columnar and basal cells with villous projections in hematoxyline and eosin stains. The ectopic ureter was inserted into the seminal vesicle cyst. The junction showed a transition of transitional epithelium to seminal vesicular epithelium (Fig. 4).
DISCUSSION
Seminal vesicle cysts occur by congenital or acquired origin. Most of them are congenital cause, which is believed to be secondary to obstruction of the ejaculatory duct. It is associated with anomalies of maldevelopment of the distal portion of the mesonephric duct, such as renal dysplasia, renal agenesis, and ectopic ureter into the seminal vesicle.8 Among the associated anomalies, ipsilateral renal agenesis was first described by Zinner. Shieh1 noted 6 cases among 119 boys who were found to have ipsilateral renal agenesis.2 In cases of seminal vesicle cysts with ipsilateral renal agenesis, the ureter may insert into the prostatic urethra or seminal vesicle.
Seminal vesicle cysts are usually asymptomatic. However, the cyst can grow and induce inflammation and stimulate surrounding viscera, resulting in bladder irritating symptoms, including urinary frequency and dysuria, suprapubic pain, hematospermia, and painful ejaculation. Initial diagnostic methods include an abdominal or transrectal ultrasonography. Abdominal computed tomography, magnetic resonance imaging, and seminal vesiculography are useful for the detection of accompanying deformity and differential diagnosis. A cystoscopy helps to confirm a hemitrigone, absence of ureteral orifice, and other anomalies in bladder.9-11
The seminal vesicle cyst is treated in patients with symptoms, and simply observation is adequate in patients without pain or functional deformity. Conventional treatment methods, including an ultrasound guided cyst aspiration and a transurethral unroofing of ejaculatory duct and seminal vesicle cyst, are limited in treatment effect compared with radical resection, and there is a great danger of reappearance or infection. Recently, a laparoscopic surgery has appeared to be most suitable for surgical treatment of seminal vesicle cyst. Laparoscopic surgery, minimal invasiveness, has advantages of direct access to the seminal vesicle with an excellent image in deep, retrovesical field compared to open resection. Also, without damage of bladder and rectum, the seminal vesicle can be dissected from the peritoneum that is covering bladder and prostate.
In 1993, Kavoussi described a principle of laparoscopic access for seminal vesicle in patient with prostatic cancer, using a five-port transperitoneal approach.13 Only 10 cases of laparoscopic excision for seminal vesicle cysts have been reported to date. Cherullo et al.12 reported 2 cases, which were treated with laparoscopic surgery in 2002. He used a four-port trasnperitoneal approach. Basillote et al.6 reported 7-year old boy with seminal vesicle cyst, who was treated with laparoscopic excision. In this case, the cyst was detected easily by filling the cyst with indigo carmine solution in laparoscopic view.
In our 4 cases, seminal vesicle cyst associated with renal agenesis was presented. They were treated with laparoscopic surgery, which was performed with a four-port transperitoneal approach. It was a feasible and effective treatment for this disease, with advantages of magnification, good visualization, direct approach, and less invasiveness. Especially, the junction of seminal vesicle cysts and remnant ureter was easily detected by an endoscopically inserted guide wire.



 XML Download
XML Download