

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Osteoporosis commonly affects most postmenopausal women, placing them at a significant risk for fractures. Alendronate has widely been used as a first line drug in the treatment of osteoporosis in postmenopausal women, because current evidence, based strictly on the principles of evidence-based medicine (EBM), suggests both the anti-fracture efficacy and safety of alendronate in postmenopausal women with osteoporosis.1-4 According to the results of randomized controlled trials (RCTs) and meta-analyses of RCTs in postmenopausal women with osteoporosis, alendronate effectively prevents vertebral, nonvertebral, and hip fractures across a spectrum of ages.1-3,5-9
Since increasing longevity in men has increased the public health burden of osteoporotic fractures in men, great attention has been paid also to male osteoporosis. Alendronate has been approved by the United States Food and Drug Administration (US FDA) for the treatment of male osteoporosis. However, the efficacy of alendronate for male osteoporosis has been less established, because there have only been a few strictly conducted RCTs on the efficacy of alendronate in men with osteoporosis.10
It is well known that hip fractures are an important cause of mortality and morbidity among elderly patients with osteoporosis.11-13 It has been established in postmenopausal women with osteoporosis that anti-resorptive therapies that produce larger decreases in bone turnover markers with larger increases in bone mineral density (BMD) are associated with greater reductions in the risk for nonvertebral fractures, especially at sites primarily composed of cortical bone.14 In particular, postmenopausal women who are treated with alendronate and show the greatest percent reduction in bone-specific alkaline phosphatase (BSAP) have the lowest risk for hip fractures, while those with the smallest reduction in BSAP have the highest risk for hip fractures.15 Alendronate-treated postmenopausal women with at least 30% reduction in BSAP have a 74% lower risk for hip fractures than those with less than 30%.15 Although the efficacy of alendronate against vertebral fractures seems to have been established in male osteoporosis,16 the efficacy of alendronate in men in relation to reduction in the risk of hip fractures remains to be established, probably because of the insufficient sample sizes for a RCT. Thus, the improvement of surrogate markers such as hip BMD and bone turnover markers is thought to be important in the prevention of hip fractures in elderly men with an increased risk for fractures.
Several studies have reported the comparative effects of alendronate or risedronate and alfacalcidol on BMD and bone turnover in Caucasian men with osteoporosis.17-20 To our knowledge, however, there are no data to show the effects of alendronate on hip BMD and bone turnover in Japanese men with osteoporosis. The purpose of this open-labeled prospective study was to compare the effects of alendronate and alfacalcidol (active control) on hip BMD and bone turnover in Japanese men having osteoporosis or osteopenia with clinical risk factors for fractures. The primary end point was hip BMD, and the secondary end point was bone turnover markers.
MATERIALS AND METHODS
Subjects
One hundred twelve men having osteoporosis or osteopenia with clinical risk factors for fractures (mean age: 71.4 years) were recruited at Keiyu Orthopaedic Hospital (Gunma, Japan) during the 27 months between January 2005 and March 2007. According to the Japanese diagnostic criteria,21,22 patients with BMD < 70% of the young adult mean (YAM) or 70 - 80% of the YAM along with a history of osteoporotic fractures are diagnosed as having osteoporosis. Patients with BMD of 70 - 80% of the YAM without any history of osteoporotic fractures are diagnosed as having osteopenia. Patients having osteoporosis or osteopenia with clinical risk factors for fractures such as current smoking, alcohol abuse (≥ 2 units a day), and a history of steroid use are treated with drugs.23 The patients in the present trial were randomly divided into two groups of 56 patients each: the alendronate (5 mg daily) group (35 patients with osteoporosis and 21 patients with osteopenia + clinical risk factors for fractures) and the alfacalcidol (1 µg daily) group (31 patients with osteoporosis and 25 patients with osteopenia + clinical risk factors for fractures). The doses indicated in the parentheses are the doses used mainly in elderly Japanese women with osteoporosis, and have been recognized as safe and effective.24-26 In particular, the dose of alendronate in Japan, which was approved by the Ministry of Health, Labor and Welfare, is half of that used in other countries according to the results of the phase II study showing that alendronate at 5 mg daily adequately suppressed bone turnover and increased lumbar BMD in postmenopausal women with osteoporosis.24 The duration of treatment was 12 months.
Preliminary screening included medical history, physical examination, plain X-rays of the thoracic and lumbar spine, hip BMD measurement, and blood and urinary biochemical tests. Subjects with a history of reflux esophagitis, gastric or duodenal ulcers, gastrectomy, or renal stone were excluded. Hip BMD was measured, and the assessment of vertebral fractures on plain X-ray films was performed as described below. The serum levels of calcium, phosphorus, alkaline phosphatase (ALP), and intact parathyroid hormone (PTH) were measured using standard laboratory techniques. The serum level of BSAP was measured with an enzyme immunoassay (EIA). The urinary level of cross-linked N-terminal telopeptides of type I collagen (NTX) was measured with an enzyme-linked immunosorbent assay (ELISA). None of the subjects had ever taken medication to treat osteoporosis prior to the present study. All the subjects were instructed to consume about 800 mg of dietary calcium daily (the minimum requirement of calcium intake in elderly Japanese) during the study period. Informed consent was obtained from each participant prior to his participation in the study.
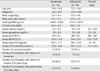
Table 1 illustrates the baseline characteristics of the study subjects. There were no significant differences in any of the baseline characteristics between the two groups (as determined by the unpaired t-test and Fisher's exact test). The past histories of the subjects that could affect bone metabolism were steroid use [asthma (n = 9), hearing loss (n = 5), and rheumatoid arthritis (n = 1)], diabetes mellitus (n = 7), hepatitis (n = 1), and cerebrovascular disease with no apparent hemiplegia (n = 3). The urinary level of NTX (normal range: 9.3 - 54.3 nM BCE/mM Cr), serum levels of BSAP (normal range: 7.9 - 29.0 U/L) and intact PTH (normal range: 10 - 66 pg/mL) tended to be higher within or above the normal ranges.27 The serum level of ALP was within the normal range (100 - 340 IU/L). After the start of the treatment, the urinary level of NTX was measured at 3 months, the hip BMD and serum levels of calcium, phosphorus, BSAP, and intact PTH at every 6 months, and plain X-rays of the thoracic and lumbar spine at the end of 12 months' treatment. We compared changes in hip BMD, urinary NTX, and serum calcium, phosphorus, BSAP, and intact PTH levels between the two groups. This protocol was approved by the Ethics Committee of Keiyu Orthopaedic Hospital.
Measurement of hip BMD
The BMD of the left total hip in the anteroposterior view was measured by dual-energy X-ray absorptiometry (DXA) using a Hologic QDR 1500W apparatus (Bedford, MA, USA). The coefficient of variation (100×standard deviation/mean) of the three measurements with repositioning within 24 hours each time was less than 1.2% in three persons.
Assessment of vertebral fractures
Plain lateral X-ray films of the thoracic and lumbar spine were obtained to detect evidence of vertebral fractures. According to the Japanese criteria, a vertebral fracture is defined according to the vertebral height on lateral X-ray films.21,22 In brief, the vertebral height is measured at the anterior (A), central (C), and posterior (P) parts of the vertebral body, and the presence of a vertebral fracture is confirmed when 1) a reduction in the vertebral height of more than 20% (A, C, and P) as compared to the height of the adjacent vertebrae is observed, 2) the C/A or C/P is less than 0.8, or 3) the A/P is less than 0.75. The assessment of vertebral fractures was performed at the T4-L4 level. This assessment was non-blinded and performed by one investigator.
Statistical analysis
Data were expressed as mean ± standard deviation (SD) in the tables and as mean ± standard error (SE) in the figures. Data were compared between the two groups by unpaired t-test. The number of patients with a history of fracture and clinical risk factors for fractures were compared in the two groups by Fisher's exact test. The significance of longitudinal changes in the parameters was determined with the one-way analysis of variance (ANOVA) with repeated measurements. The longitudinal changes in the parameters were compared between the two groups with the two-way ANOVA with repeated measurements. All statistical analyses were performed using the Stat View-J5.0 program on a Windows computer. A significance level of p < 0.05 was used for all the comparisons.
RESULTS
Adverse events
Eleven patients (19.6%) in the alendronate group and 14 patients (25.0%) in the alfacalcidol group discontinued treatment during the 12-month-period. The main reasons for the dropouts from the study were epigastric pain (n = 8) and difficulty with compliance (n = 3) in the alendronate group, and epigastric pain (n = 3), difficulty with compliance (n = 10), and surgery for osteoarthritis of the knee (n = 1) in the alfacalcidol group. No serious adverse events necessitating hospitalization were observed in either group. Thus, the trial was successfully completed in 45 (80.4%) patients in the alendronate group and 42 (75.0%) patients in the alfacalcidol group, and the data from a total of 87 patients (77.7%) were included in the analyses.
There were no significant differences in any of the baseline characteristics between 45 patients in the alendronate group and 42 patients in the alfacalcidol group who completed the 12-month trial.
Changes in serum and urinary biochemical markers and hip BMD
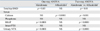
With regard to the percent changes (mean ± SE) in the urinary level of NTX at 3 months, the urinary level of NTX was significantly decreased (-46.4 ± 2.9%) in the alendronate group, but did not change significantly (+13.2 ± 12.5%) in the alfacalcidol group (one-way ANOVA with repeated measurements, Table 2). There was a significant difference in changes in the urinary level of NTX between the two groups (two-way ANOVA with repeated measurements, Table 2).
Fig. 1 shows the longitudinal changes in the serum levels of calcium, phosphorus, BSAP, and intact PTH. The serum level of BSAP was significantly decreased (-27.5% at 6 months and -34.1% at 12 months), but the serum levels of calcium (-1.1% at both 6 and 12 months), phosphorus (-3.3% at 6 months and -4.2% at 12 months), and intact PTH (+7.1% at 6 months and +7.6% at 12 months) did not significantly change in the alendronate group (one-way ANOVA with repeated measurements, Table 2). On the other hand, the serum level of calcium increased significantly (+1.5% at 6 months and +2.2% at 12 months), but the serum levels of phosphorus (+1.3% at 6 months and +0.5% at 12 months), BSAP (+1.4% at 6 months and +1.8% at 12 months), and intact PTH (-6.3% at 6 months and -7.5% at 12 months) did not significantly change in the alfacalcidol group (one-way ANOVA with repeated measurements, Table 2). There were significant differences in changes in the serum calcium and BSAP levels between the two groups (two-way ANOVA with repeated measurements, Table 2).
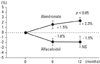
Fig. 2 shows the longitudinal changes in total hip BMD. The BMD increased significantly (+1.5% at 6 months and +2.3% at 12 months) in the alendronate group, but did not significantly change (-1.8% at 6 months and -1.9% at 12 months) in the alfacalcidol group (one-way ANOVA with repeated measurements, Table 2). There was a significant difference in changes of BMD between the two groups (two-way ANOVA with repeated measurements, Table 2).
DISCUSSION
A prospective head-to-head trial was conducted to compare the effects of alendronate and alfacalcidol (active control) on hip BMD and bone turnover in Japanese men with osteoporosis or osteopenia with clinical risk factors for fractures. The focus of the discussion was whether alendronate would successfully increase hip BMD following reductions in bone turnover markers, including serum BSAP and urinary NTX, compared with alfacalcidol (active control). Because of the small sample size of men with an increased risk for fractures, the assessment of surrogate markers such as hip BMD and bone turnover markers may be important from the point of view of the prevention of hip fractures in men having osteoporosis or osteopenia with clinical risk factors for fractures.
The higher risk of osteoporotic fractures in men is considered to accrue from a lower peak volumetric BMD and greater bone loss with aging, particularly in those subjects with risk factors, hypogonadism, or underlying illness.28 It is likely that bone formation, as reflected by bone formation markers, decreases with aging and in the presence of fractures in men.28 On the other hand, bone resorption, as reflected by bone resorption markers, may increase in late life, probably reflecting increased bone turnover associated with secondary hyperparathyroidism.28 However, it still remains controversial as to whether male osteoporosis is caused mainly by increased bone resorption, even though increased or decreased bone turnover has been reported in men with vertebral fractures.29,30
In the present study, twenty-six patients (23.2%) had illnesses that could affect bone metabolism, and the urinary level of NTX and serum levels of BSAP and intact PTH at the baseline tended to be higher within or above the normal ranges. Thus, anti-resorptive drugs might have been expected to be efficacious in our subjects.
Alfacalcidol is known to suppress bone resorption and maintain or even increase bone formation, suggesting that alfacalcidol supercouples bone formation and resorption.31 Alfacalcidol suppresses the synthesis and release of PTH and increases the intestinal absorption and reabsorption of calcium in the distal renal tubules.32 In rats, alfacalcidol has been shown to improve the microarchitecture and strength of bone.31,33 Vitamin D supplementation appears to reduce the risk for falls among ambulatory or institutionalized older individuals with stable health by more than 20%.34 In the present study, alfacalcidol, an active control drug, sustained total hip BMD (-1.9% at 12 months) as well as the urinary level of NTX (+13.2% at 3 months) and serum level of BSAP (+1.8% at 12 months) in men with an increased risk for fractures, although we did not assess the incidence of falls. Because of the similar baseline bone turnover status in two different categories such as osteoporosis and osteopenia + clinical risk factors for fractures, the BMD change during 12-month treatment was similar in the two categories (data not shown). Higher bone turnover tended to cause a reduction in total hip BMD, but the BMD loss was not statistically significant, probably due to the small sample size and short-duration of the study. These effects of alfacalcidol seem to be less pronounced compared with those of previous studies in Caucasian men with osteoporosis.17,18 One possibility is that alfacalcidol might be less effective in our subjects, probably because of the smaller number of patients with vitamin D insufficiency or deficiency as indicated by the serum level of ALP.35
On the other hand, alendronate increased total hip BMD (+2.3% at 12 months) following reductions in the urinary level of NTX (-46.4% at 3 months) and serum level of BSAP (-34.1% at 12 months). Because of the similar baseline bone turnover status in two different categories such as osteoporosis and osteopenia + clinical risk factors for fractures, the BMD change during 12-month treatment was similar in the two categories (data not shown). These changes were significantly different between the alendronate and alfacalcidol (active control) groups, suggesting the efficacy of alendronate for hip BMD and bone turnover in men having osteoporosis or osteopenia with clinical risk factors for fractures. In other words, alendronate improved surrogate markers in relation to hip fractures in men with an increased risk for fractures. The effects of alendronate on hip BMD and bone turnover markers seemed to be compatible with those in Caucasian men with osteoporosis.10,16,18,19 Because each 1 standard deviation reduction in a 1-year change in BSAP is associated with 39% fewer hip fractures in alendronate-treated postmenopausal women,15 a reduction in the serum level of BSAP (-34.1% at 12 months) could possibly contribute to a reduction in the incidence of hip fractures in our subjects.
A randomized, double-placebo, double-blind clinical trial conducted over a duration of 18 months' among patients with a rheumatic disease who were starting glucocorticois showed that total hip BMD was increased by 0.8% in the alendronate group and decreased by 2.2% in the alfacalcidol group.36 Alendronate suppressed bone resorption and increased serum PTH levels, while alfacalcidol slightly increased bone formation.36 These results suggested that alendronate was more effective in the prevention of glucocorticoid-induced bone loss than alfacalcidol, in agreement with our results.
Eleven patients (19.6%) in the alendronate group dropped out from the study, and the main reason for the dropouts was gastric problems. Adverse upper gastrointestinal (GI) symptoms are considered to be the most significant adverse effects of alendronate in clinical practice, even though RCTs show no statistically significant difference in the incidence of adverse upper GI events between men with osteoporosis treated with alendronate and a placebo.10 Increased sensitivity for the detection of upper GI symptoms in the study subjects might have been more likely than the existence of a causal relationship between upper GI symptoms and alendronate.
On the other hand, 14 patients (25.0%) in the alfacalcidol group dropped out from the study, and the main reason for the dropouts was difficulty with compliance. The worrisome adverse effect associated with alfacalcidol may be hypercalcemia, because this drug stimulates intestinal calcium absorption. In the present study, the serum level of calcium trended to increase (+1.5% at 6 months and +2.2% at 12 months) from the baseline (the mean value: 9.0 mg/dL). However, no patients experienced renal dysfunction, including acute renal failure, due to hypercalcemia. No case of hypercalcemia was documented in men treated with alfacalcidol (1 µg daily) in a previous study.18 Probably because of insignificant changes in BMD and bone turnover markers during the treatment, adherence to alfacalcidol might have been worse than that to alendronate, resulting in a larger number of patients who discontinued the trial due to noncompliance.
There were some notable limitations of this study. Firstly, the study was not a double-blind trial, but an open-labeled study. Therefore, some of the results might have been biased. Second, the number of study subjects was relatively small and not sufficient large enough to lend sufficient power to the results. Third, although all the subjects were instructed to consume about 800 mg of dietary calcium daily during the study period, it remains uncertain how much calcium was actually consumed by the subjects. Thus, double-blind randomized placebo-controlled studies conducted on a sufficient number of subjects under sufficient calcium supplementation are needed to confirm the present results.
In conclusion, the present prospective head-to-head trial showed that alendronate increased total hip BMD, followed with reductions of the urinary level of NTX and serum level of BSAP, while alfacalcidol sustained total hip BMD and the urinary level of NTX and serum level of BSAP. The study confirmed also the greater efficacy of alendronate than alfacalcidol (active control) in increasing hip BMD and reducing bone turnover in Japanese men having osteoporosis or osteopenia with clinical risk factors for fractures.

 XML Download
XML Download