

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lens particle glaucoma is a form of lens-induced open-angle glaucoma; and it is characterized by the release of lens material, obstruction of the trabecular meshwork by swollen macrophages and increased resistance to aqueous outflow.1-3 Some authors described the blockage of drainage channels by macrophages that had engulfed lens proteins as well as blockage by the cortical fluid that had escaped the ruptured lens capsule.4,5 This disorder may be precipitated by penetrating lens injury, cataract extraction or Nd:YAG laser posterior capsulotomy.1,6 However, dehiscence of the lens capsule without penetrating trauma or surgery is a rare cause. Here in, we report an unusual case of lens particle glaucoma that occurred after a spontaneous anterior capsular dehiscence.
CASE REPORT
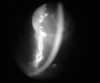
A 66-year-old male presented with a history of sudden ocular pain and redness in OD for 10 days. The patient had a history of a hypermature cataract in the right eye 7 years previously. He denied recent trauma in OD. No inflammatory antecedents were reported. Best corrected visual acuity in OD was hand motion close to the face, while OS was 0.8. Slit lamp examination of OD showed conjunctival congestion, moderate corneal edema and a deep anterior chamber with lens particles at the inferior angle (Fig. 1). There was a chamber reaction with flare (2+) and cells (2+). Numerous large white flecks were observed circulating in the aqueous. Lens cortex material was noted to protrude through the dehiscence site of the anterior capsule. The pupil was mid-dilated and adhered to the disrupted anterior lens capsule. The lens showed the presence of a hypermature cataract.
The intraocular pressure (IOP) measured with Goldmann applanation tonometer was 55 mmHg in OD and 17 mmHg in OS.
Gonioscopy with Goldmann 2-mirror goniolens demonstrated the presence of wide-open angles and lens particles that were thickly attached to the inferior trabecular meshwork (Fig. 2). There was no sign of angle recession, and no corneal or scleral perforation was noted in OD. Following dilation of the pupils, slit lamp examination of the anterior segment showed fragmented lens particles protruding through the ruptured anterior capsule margin. Evaluation of the anterior capsule of the lens showed that there was a pre-existing anterior capsular dehiscence, extending along the pupillary margin. This was associated with an intracapsular distension, and protrusion of the anterior sub-capsular lens particles through the dehiscence into the anterior chamber. Phacodonesis was not observed. The fundus was invisible due to the hypermature cataract. The examination of the left eye was within normal limits. Ultrasound B-scan of the right eye was within normal limits.
A diagnosis of right eye lens-particle glaucoma was made. Medical therapy for the elevated IOP included 250 mL of 20% mannitol (1 g/kg body weight) intravenously over 45 minutes in the acute phase, followed by Acetazolamide 250 mg tablet four times daily, Dorzolamide 2%/timolol 0.5% eye drops twice daily and brimonidine 0.15% eye drops twice daily for maintenance of IOP control. Cataract surgery was recommended for the treatment of lens-particle glaucoma. An anterior chamber paracentesis was performed, and a 0.2-mL sample of the white material in the aqueous was obtained.
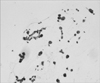
The patient underwent an extracapsular cataract extraction. A posterior lens capsule rupture which might have been produced during surgery was confirmed intraoperatively. Anterior vitrectomy was performed with an automated vitrector (Alcon. Accurus® 400VS) for the vitreous prolapse and for the removal of the sticky cortical matter in the anterior vitreous and anterior chamber angle. Histological examination of the anterior chamber aspirate revealed lens cortical fibers, numerous hemosiderin laden macrophages and neutrophils (Fig. 3). No bacterial analysis, florescence stain or culture with the aqueous humor sample was done.
Postoperatively, the patient was treated with topical moxifloxacin 0.5%, prednisolone 1% eye drops in a tapering dose regimen and atropine 1% eye drops twice daily for 2 weeks. At the 1-month postoperative follow-up, the right eye IOP was 16 mmHg without any intraocular antihypertensive medication.
DISCUSSION
Generally, lens particle glaucoma has been reported to occur after cataract extraction7 or penetrating lens injury.8 It is believed that an advanced cataract alone rarely ruptures spontaneously.1 This is an uncommon clinical variation of lens particle glaucoma, however, spontaneous rupture of the anterior lens capsule developed without a lens injury in this case, and there was no clinical evidence of trauma or infection that could lead to dehiscence of anterior capsule.8 The event precipitating the release of lens material in this patient was presumably dehiscence of the anterior capsule due to the expansion of the lens bag in the hypermature cataract. An earlier report showed that absorption of aqueous, hydration of the cortex and increased intralenticular swelling result in spontaneous rupture of the anterior capsule and the release of lens particles9: Through a breach in the integrity of the capsule, aqueous humor can hydrate the cortex, resulting in the release of lens material into the anterior chamber causing uveitis and glaucoma. By perfusing the entire enucleated human eye with particulate lens material, the aqueous outflow was found to decrease in a linear fashion as the concentration of lens particles increased.10
For patients with lens particle glaucoma, the medical therapy is similar to that used for primary open angle glaucoma.9,11-13 In order to dilate the pupil, cycloplegics can be applied, however the miotics should be avoided due to increase formation of synechiae in these cases.1 Topical corticosteroids are used to treat inflammation. Therefore, the doses of steroid administered should be titrated in order to reduce the inflammatory response and synechiae, while allowing the retained lens material to resolve.9 Intensive steroid therapy might delay absorption of the lens material. When the pressure cannot adequately be controlled despite medical therapy, the residual lens material should surgically be removed promptly.1,4,12 A delay of surgery may allow the lens material to remain trapped within the capsule or the inflammatory membranes.9
Based on the results of a VDRL (+), the patient was diagnosed with late stage latent syphilis during routine laboratory testing for surgery. Although the aqueous humor was not analyzed, uveitic origin was not ruled out. It is unlikely that this was related to the lens particle glaucoma.
To our best knowledge, lens particle glaucoma secondary to a spontaneous anterior capsular dehiscence without trauma has not previously been reported. Surgical removal of the lens material usually controls the high IOP, and the need for additional glaucoma surgery is not common.

 XML Download
XML Download