

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Medical education has been focused on delivering biomedical knowledge and creating skillful doctors and, in the process, has overlooked the importance of the art of the healer.1-3 When dealing with the issues of educating true healers and professionals, the first thing to consider is whether we are selecting students who have the potential to be good doctors. When selecting medical students, we should look for students whom are patient-oriented and have a passion for the profession, not just good academic grades and good memorizing skills. To do this, we need to understand beforehand the factors of medical professionalism that should be required in medical school applicants.
There have been many studies on medical professionalism, but it has not been easy to come to a common definition.4-6 This is because although it may be said that the foundation of medical professionalism is universal, the attributes of a doctor may differ between countries with distinct medical histories.7,8 Furthermore, the definition of medical professionalism tends to change with time. In December 2005, the Royal College of Physicians made available a report titled 'Doctors in Society: Medical Professionalism in a Changing World' which described UK's new definition of medical professionalism and its principles.9 The definition given in this report is: "Medical professionalism signifies a set of values, behaviors, and relationships that underpin the trust the public has in doctors. Thus, in their day-to-day practice, doctors are committed to integrity, compassion, altruism, continuous improvement, excellence, and working in partnership with members of the wider healthcare team." We should note here that the report also stresses some previously-defined aspects of professionalism that should be abandoned, these being mastery, autonomy, and self-regulation.10-16 One of the many examples of these aspects is the Canadian Medical Association's policy which specifies that the three major features of medical professionalism that benefit society are 'the ethics of service, clinical autonomy, and self-regulation'.17 Such examples illustrate that the concept and the essential elements of medical professionalism can differ due to culture and era.
In abundance are articles with respect to medical professionalism.6,18-22 However, less has been written about the specific elements of medical professionalism that medical school applicants should have, which may be a very important factor in student selection. It also would be very important to see if entering medical students themselves actually carried these core elements. We found no previous research that had determined the core elements of medical professionalism using the Delphi survey, nor any articles that had examined the level of professionalism in those recently accepted to medical school, nor any articles that had analyzed whether medical students and medical school professors possess different opinions on the level of professionalism in medical students.
The primary concern of this study was to examine the core elements of medical professionalism in students entering medical school in Korea. More specifically, the study set out: 1) to determine the core elements of medical professionalism in medical school applicants, 2) to examine the level of professionalism in medical students newly entering medical school, and 3) to analyze the perceived differences in the level of professionalism in medical students between medical students themselves and professors.
MATERIALS AND METHODS
In order to achieve the above purposes, 250 medical school professors were chosen for the Delphi survey and 250 first year medical students who had just entered medical school were asked to complete a written questionnaire created from the final results of the Delphi survey.
A large number (250) was chosen for our panel because the Delphi survey was designed to be repeated 4 times, and we expected a notable loss of our panels for 2 reasons. They were selected from medical school faculties, who seem to be quite busy, and 1 of the inherent features of the Delphi is its very low response rate. For our panel, 100 members were randomly sampled by the 'Korean Medical School Statistics (2004-2005)'.23 There are 41 medical schools in Korea, and all current information on these medical schools, including a list of medical professors, are stated in this book. An additional 100 were selected by the members of ten medical education departments at ten medical schools. Each individual medical education department selected 10 professors from their school who were thought to be able to answer the Delphi questions 'without much difficulty'. This was done because medical professionalism is still a very controversial subject in Korea and many faculty members are unfamiliar with the word itself. The remaining 50 members were randomly sampled using the list of 700 members from The Korean Society of Medical Education. All the panel members were asked to state their 'understanding of the word, medical professionalism' and their position at their medical school as the basis of their expertise on the subject of medical professionalism.
In the first round of the survey, the response rate was 42% (106 respondents). Using this number, second, third, and fourth surveys were done. The second round of the Delphi survey had a 48% response rate (51 respondents), the third Delphi survey 51% (54 respondents), and the fourth Delphi survey 43% (45 respondents), which averaged to a response rate of 46%. The panel's 'level of understanding of medical professionalism' used a 1-7 Likert scale to see a clear distinction between the experts and the non-experts. The mean was calculated at 5.0, showing that the panel members were sufficiently fit to answer the survey. The Delphi survey started in May 2005 and it took six months to complete all four rounds.
The other major portion of the study's purpose was the medical school students. We considered the location of each of the 41 medical schools in Korea, and 2 schools were chosen from the capital city and 1 from the provinces. From these 3 schools, the entire population of 250 first year medical students was asked to answer a questionnaire. The response rate was 92% (230 respondents). One response was not appropriate for the study and 229 responses were finally used in the analysis. The questionnaire was done in March 2006, which is the beginning of a new school term in Korea, so that they could represent current medical school applicants.
Instruments
Two instruments were used in the study. One was the Delphi survey, which was used to determine the core elements of medical professionalism in medical school applicants, and the other was the written questionnaire, which was used to examine the level of professionalism in medical students who were just entering medical school.
Delphi
Using Delphi as a method to define core elements of professionalism offers many advantages. It is standard for the experts' identities and responses to be anonymous to all but the researcher with the Delphi.24 This allows experts to express their opinions honestly. Another major advantage is that it allows geographically diverse groups of experts to be used, and the repeated rounds of the survey, with each utilizing the data from the previous round, allow panelists to consider areas they may not have thought of previously and possibly to revise their opinions. This gives a Delphi consensus the advantage of strong validity.25 Our research focused on defining the core elements of professionalism in a national level, which needed a diverse group of experts.
The first round of the Delphi asked the panel in open question form to brainstorm on 'the elements of medical professionalism that medical school applicants should have'. A simple guide was given for the panel to list these elements into the domains of 'dealing with others', 'dealing with oneself', and 'others', which was partly adopted from Luijk's classification18 of the elements of medical professionalism. Unfortunately, this guideline was not very effective as the result revealed similar elements in different domains which showed inconsistency, and some responses from the panel pointed out that this classification was too obscure. As a result, the elements produced from the first round of Delphi were reclassified as 'professional knowledge', 'professional skills', and 'professional attitude'. This classification was then further divided into eight subordinate categories.
This process of segmentation and classification was fully revised by the panel through a second and third cycle of the Delphi survey. The second cycle asked whether the classification of the elements of medical professionalism into 3 domains and eight categories was appropriate, and the panel could correct or eliminate classifications as it saw fit.
The third cycle reviewed the results of the second cycle; the panel was asked to score the importance of each element and the level of corresponding elements of the entering students using the 1-5 Likert scale which is the most common Likert scale. The result of this cycle was revised during the final round of the Delphi survey so that the panel could come to a mutual agreement. If a panel member wished to disagree with the mean score, they were asked to state the reason. At the final round, students' professionalism scores were given by the professors which were based on their general observations of previous groups of students entering medical school.
Questionnaire
A questionnaire was prepared on the basis of the Delphi survey results, for the 250 new medical students from the three chosen medical schools. The questionnaire asked the students to self-score their own perceived level of each of the elements of professionalism. The questionnaire consisted of 27 questions categorized into 'professional knowledge' (3 questions), 'professional skills' (12 questions), and 'professional attitude' (12 questions).
Data analysis
During the third Delphi survey, the 1-5 Likert scale was used for some of the questions. The reliability of the student questionnaire used Cronbach's Alpha figures, which was 0.87 in 'professional knowledge' and 0.90 for the other 2 domains.
In order to determine the core elements of medical professionnalism in medical school applicants, we sorted through the data for many hours to obtain the first Delphi survey result. In total, 1,580 elements were classified into three larger umbrella domains and eight subordinate categories; we were then able to analyze the domain and category frequencies during the second Delphi survey. During the third and fourth Delphi surveys, descriptive statistics were done to find the mean, standard deviation, the maximum and minimum levels of importance, and the current level of professionalism in the entering medical students as judged by the panel.
The analysis of the level of professionalism of the entering students was also done by descriptive statistics calculating the mean and standard deviation. To analyze the difference between the scores given by medical students and those given by professors on the level of professionalism in medical students, the independent t-test was used.
RESULTS
Core elements of medical professionalism for medical school applicants
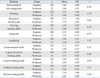
From the first Delphi survey, 1,580 elements were collected. After exhaustive hours of sorting, the elements were then reclassified into 3 domains, 'professional knowledge', 'professional skills', and 'professional attitude'. This classification was then further divided into eight subordinate categories and finally readjusted into 27 core elements. Table 1 shows the 27 core elements of medical professionalism.
The 'professional knowledge' domain was classified into 2 subordinate categories; 'understanding basic science', and 'understanding human-social science'. These subordinate categories contained three core elements including 'knowledge of basic science', 'basic knowledge of human-social science', and 'understanding the characteristics of the Korean society'.
The 'professional skills' domain was classified into 3 subordinate categories including 'management skills', 'human relationships', and 'multiple thinking skills'. Each of these 3 subordinate categories was more specifically classified into 12 subordinate elements; 'self-restraint and risk management', 'planning', 'physical and mental health', 'life-long learning skills', 'teamwork', 'leadership', 'communication skills', 'foreign language skills', 'logical and critical thinking skills', 'creative thinking skills', 'problem solving skills', and 'decision-making skills'.
In the 'professional attitude' domain, 'service attitude', 'monitoring attitude', and 'progressive attitude' categories were defined. This subordinate categories was classified into 12 subordinate elements; 'service oriented', 'respect for others', 'humanity', 'etiquette', 'ethical thinking and behavior', 'self-confidence', 'integrity', 'sense of duty', 'self-examination', 'religious and dilettante life', 'open and positive mind', and 'appearance'.
Level of medical professionalism in students entering medical school
The level of 'medical professional knowledge' in the first year medical students was 2.63, 'professional skills' 3.23, and 'professional attitude' 3.36. These means were derived from the students' self-rated scores, and the overall mean score was 3.22.
Table 1 shows the level and rank of importance of the 27 elements allotted by the Delphi panel. The element with the highest score was 'lifelong learning skills' (M = 4.57); 'ethical thinking and behavior' (M = 4.40) ranked second; 'service oriented' (M = 4.36) was third; and 'respect for others'(M = 4.36) fourth. The next five elements (ranking 5th to 10th) were: 'communication skills', 'self-restraint and risk management', 'sense of duty', 'knowledge of basic sciences', 'foreign language skills' and 'problem-solving skills'. The 2 elements under 'understanding human-social science' in the 'professional knowledge'domain ranked 25th and 26th. Most of the top-ranking elements were from the 'professional skills' and 'professional attitude' domains.
Difference in recognition of the level of professionalism in medical students
Table 2 shows the analyzed result of the differences in the recognition of the levels of professionalism in medical students between medical students and professors. According to these results, there was no difference in the 'professional knowledge' domain but differences were seen under 'professional skills' (t = 6.23, p < 0.001) and 'professional attitude' ( t = 7.29, p < 0.001). In both these domains, the mean score of the students were higher than that of the professors. The overall mean score showed the same propensity. The total mean score of the students was slightly above average (M = 3.22), whereas the score given by the professors (2.71) was below the average score, showing a clear discrepancy in this recognition (t = 6.88, p < 0.001) between the 2 groups.
Differences in professional knowledge elements
There was no difference shown under 'professional knowledge' (Table 2). But it should be noted that students and professors both felt that students lack professional knowledge. Professors pointed out that the students were lacking in the areas of 'basic knowledge of human-social science' (M = 2.15) and 'understanding the characteristics of Korean society' (M = 2.17) compared to the 'knowledge of basic science (M = 3.15)' which is the foundation for learning basic medical knowledge.
Differences in professional skills elements
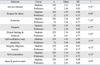
Table 3 shows the differences in the recognition of professional skills in medical students between medical students and professors. Except for the element of 'foreign language skills', there were significant differences in all other elements. Large differences were seen in 'self-restraint and risk management' (t = 6.16), 'teamwork' (t = 6.93), 'communication skills' (t = 5.27), 'logical and critical thinking skills' (t = 5.46), 'problem-solving skills' (t = 5.51), and 'decision-making skills' (t = 5.44). The mean scores of these elements were higher in the students' assessment.
Differences in professional attitude elements
The differences in the recognition of professional attitudes in medical students between medical students and professors are shown in Table 4. Among the twelve elements of professional attitude, the nine values were significantly different. Notable differences were shown in 'respect for others' (t = 8.00), 'humanity' (t = 7.10), 'etiquette' (t = 6.77), 'ethical thinking and behavior' ( t = 5.52) and 'service-oriented' (t = 5.21). The difference in mean scores for 'respect for others' was 0.95, 'etiquette' 0.88, and 'humanity' 0.82.
Differences in ten medical professionalism core elements
The 10 medical professionalism core elements and their comparisons are described in Table 5. One distinctive result is that the most important medical professionalism element to medical school applicants is 'life-long learning skill', but the students' self-assessment of this element ranked it 17 (mean score 3.30) among the total 27 elements. Further, the professors ranked this same element 14th (mean score 2.69). 'Ethical thinking and behavior' was ranked second in importance overall. Students thought that this element was their strongest quality (ranked first in mean score), but the professors thought otherwise (ranked 8th). Similar results were seen for 'respect for others' where the students' self-assessment score was 3.49 (ranking 2nd in mean score) but the professors' mean score of the students was 2.54, ranking the element 20th. Having a 'service-oriented' mind and behavior are very important traits for doctors, and this element ranked fourth in importance. However, assessments from both students and professors of the students' level were low (ranking 20th and 24th, respectively, in mean score ranking).
In summary, the recognition of professionalism in medical students between medical students and professors showed significant differences. More specifically, there were significant differences in 'professional skills' and 'professional attitude'. Of 27 elements, significant differences were shown in 20. And in all these differences, students' mean scores were higher than those of the professors.
DISCUSSION
Interestingly, the core elements of medical professionalism for medical school applicants were reclassified into the 3 domains of 'professional knowledge', 'professional skills', and 'professional attitude'. Not many previous studies specifically delineated 'professional knowledge' as a core element but similar concepts can be found in studies such as Monekosso26 and Wagner et al.27 Monekosso divided the 'doctor-patient relationship' learning model into 4 categories- 'professional thinking', 'professional attitudes', 'professional skills', and 'professional knowledge'. A very recent study on defining medical professionalism by Wagner et al. determined the areas of congruence and difference in medical professionalism, and one of the three primary themes was 'medical knowledge and technical skill'. Baik28 also mentions that professional medical education can be divided into 'accumulation of professional knowledge and its practical application' and 'professional behavior'.
Although we may see similarities, the major reason for having differences between what is considered medical professionalism in western cultures and Korean is due to the different historical background of development of medical professionalism. Korea has accepted Western medical education since the late 19th century, but the actual development of the medical profession was completed by using the Japanese medical system.29 Physicians were protected by the government and had a very high social- economic status along with professionals in law and education. These professions required no struggles for either autonomy or higher social status or to form a strong union in institutional level. This caused physicians to exhibit individualism or self-centeredness to some extent and these physicians often lacked the internal self-regulated motivation.29-32 They were less interested in forming positive relationships with local societies and reacting to the societies' needs.33 Such phenomenon still exists in the medical system, and some of these aspects can be seen in the results of this study where many of the selected elements are about doctors themselves, and the doctors' are cultivating their own qualities. These results also suggest a lack of interest in professional attributes such as self-regulation and autonomy (including patient-autonomy).
On the other hand, western cultures have various institutions such as the Association of American Medical Colleges (AAMC), the American Board of Internal Medicine (ABIM), the Accreditation Council for Graduate Medical Education (AGCME) in the US, and the European Federation of Internal Medicine (EFIM) in Europe, the General Medical Council (GMC) and the Royal College of Physicians in the UK, which are all very interested in dealing with medical professionalism at a national level. The US for instance has reexamined the country's professional ethics since 1990s.34 Demonstrating interest and reflection on their professionalism, ABIM and EFIM collaborated to work on their members' professionalism and came up with the 'Charter on Medical Professionalism' by 2002.35,36 Here, the primacy of patient welfare, patient autonomy, and social justice were the 3 major principles. AAMC's 'Physicians for the 21st century' underscored altruism, integrity, caring and compassion, respect, accountability, excellence in scholarship, and leadership.37 ACGME's core elements of professionalism were respect, compassion, integrity, responsiveness to needs, altruism, accountability, commitment to excellence sound ethics, and sensitivity to culture, age, gender, disabilities.38 As mentioned in the introduction, many of these American medical professionalism competencies can be found in other countries' professionalism also. But the UK's Royal College of Physicians' report abandoned mastery, autonomy, and self-regulation attributes because the association regarded them as no longer a significant professional marker in the UK.9 But from the result of our study, the Korean doctors still think that the mastery of professional knowledge, autonomy, and self-regulation are the core qualities of medical professionalism. Professional skills such as 'foreign language skills' and 'understanding the characteristics of Korean society' are cultural specific elements.
It is a very big step forward that we defined 27 core qualities of medical professionalism including 'honesty', 'self-regulation', 'integrity', and 'respect for others' where these qualities were not found in any of Korean medical schools' educational objectives before.39 Most of Korean medical schools' educational objectives had been related to 'accountability', 'medical ethics' and 'service oriented mind'. Finding 'life-long learning skills', 'ethical thinking and behavior', 'respect for others', 'service-oriented', and 'communication skills' in top five qualities of medical professionalism may be the result of the changes and trends in patient expectations and doctor-patient relationships in Korea. Healthcare service in Korea is no longer independent care given by 1 individual, but a teamwork and collaboration of various professions.4 The movement of consumerism in the healthcare system after the 1970s have also effected the relationship between doctors and patients, and have challenged the authority of doctors' professions.40 Along with the changes in the healthcare society, the traditional and hierarchical medical curriculum, called the Flexnerian curriculum, have also gradually changed into a more integrated curriculum of basic and clinical medicine.41 Medical educators in Korea have adopted much from the 'SPICES Model' which means that it is student centered, problem-based, integration, community-based, elective courses, and systematic education.41,42 In 2000, The Korean Council of Deans of Medical College released the report named 'The 21st century Korean Medical Education Plan: the 21st century Korean Physicians'34 which addressed the importance of life-long learning skills, problem-solving skills, and knowledge of basic medical science as the primary principles of Korean medical education. Therefore, from the results of this study, it can be said that there are some attributes or qualities that are culturally specific and there are some qualities that are universally accepted as medical professionalism.
Another important issue which we can talk about in light of the results is the question of whether high levels of professionalism are necessary for entering Korean medical schools. Although the 27 elements of medical professionalism required for students entering medical schools are defined to be the core competencies which medical school professors think that the students should carry before entering the medical school, the results show that professors are not quite satisfied with the entering students' professionalism level. Then, we should either focus on selecting students with higher professionalism levels required for entering students or investigate whether these required competencies are taught and learned during their medical education to finally reach the level of satisfaction. From past research that I have done, I have found that by the time of graduation, medical students showed an overall increase in all 3 domains of medical professionalism, especially in 'professional attitude'.39 Their scores, however, did not reach more than average. There are a number of references indicating effective ways in which these competencies can be taught in medical school. Kasar and Clark43 argued that professional behaviors must be developed and nurtured because they embody what it takes to be successful as a professional. It is part of our responsibility for fostering professional socialization as practitioners and educators. Kasar and Clark43 also believed that professionalism requires specific knowledge, attitudes, and values, and that these behaviors are dependability, professional presentation, initiative, empathy, cooperation, organization, clinical reasoning, supervisory process, verbal communication, and written communication. And they suggested effective approaches to teach and learn these professional behaviors. For example, community service initiatives, group projects, peer reviews, reading about disability experiences, role models, writing journals or diaries, and watching videos about disability experiences are effective ways to teach and learn empathy. For communication skills, they suggested debates, faculty assistantships, interdisciplinary and multidisciplinary projects, marketing projects, peer reviews, simulated case conferences, student lecture presentations, student involvement in writing and research activities of faculty, verbal defense of position papers, poster presentations, student portfolio, written case histories, etc. Although professionalism is a very complex subject, our review8 and the Wear and Aultman44 review describes numerous examples of US medical schools' professionalism courses that explain the schools' effective ways to teach professionalism, white coat ceremonies, using trigger films, peer review and self-reflection, community service initiatives programs, leadership programs, case study, etc. Therefore, it can be said that, although high levels of professionalism are recommended for entering medical school, students actually getting into medical schools did not already possess these levels yet. As they are the competencies which must be developed and enhanced throughout the students' entire developmental process,43 many medical schools are trying to provide effective ways to teach and learn medical professionalism.
Prominent differences in the recognition of the level of professionalism in medical students by students and by professors were found in 23 elements (85%). With the students' scores being higher than the professors', this indicates that either the students are overestimating themselves or that the professors are underestimating their students. Whichever the reason, it is clear that students do not meet the expectations of the professors. Most of the assessment scores given by the professors were below average. This implies that there needs to be a concrete plan on how to raise students' professional competencies and attributes through medical education since these students are accepted in medical school. It would be useful to do further studies to investigate whether these knowledge, skills, and attitudes improve and whether they are maintained throughout medical school. Peer assessments and evaluations on medical professionalism can be done continuously, and as Papadakis et al45 pointed out, the sooner the better.
Limitations of this research include the Delphi method, and in particular the panel, which could have been expanded to include patients and physicians in community practice. There could be some problems with generalization of the questionnaire results as the subjects were limited to 3 medical schools.
In addition, the researchers also recognize that some areas require further research. Defining medical professionalism or evaluation of the elements of medical professionalism can be done at individual medical schools or by assembling focus groups where many medical schools and organizations can participate.4 Doing this in each country is very important since, as the study pointed out earlier, each country has its own unique medical history background and culture affecting the defined qualities, competencies, and attributes of a 'good doctor'. Thus, using a focus group gives a consensus result and a guideline for individual schools as they develop and evaluate their medical professionalism curriculum.
In conclusion, there were elements of medical professionalism that were asked for medical school applicants, and such qualities can be summarized into 27 elements and categorized into three domains; professional knowledge, professional skills, and professional attitude. The levels of these elements were above average (self-assessed by the students) and most of the top-ranking elements were from the 'professional skills' and 'professional attitude' domains. There were prominent differences in the recognition of the levels of these elements in medical students by medical students and by medical school professors. Further studies investigating the reasons for discrepancy are needed.



 XML Download
XML Download