

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recent studies have shown that exposure to second-hand smoke during pregnancy, which has been referred to as environmental tobacco smoke in the past, is associated with the increasing risk of adverse pregnancy outcomes such as delayed fetal growth, fetal mortality, preterm delivery, and low birth weight.1-4 According to the Surgeon General's Report, the term "second-hand smoke" is considered to better capture the involuntary nature of the exposure.5 In those studies, the assessment methods for exposure to second-hand smoke were largely divided into a self-reported assessment of exposure using a questionnaire and an objective assessment of exposure using a biomarker such as cotinine. The latter is considered to be more accurate and objective for exposure to second-hand smoke.
Previous studies have reported the agreement between self-report and biomarker estimation with regard to exposure to second-hand smoke among pregnant nonsmokers.6-10 Among those studies, Rebagliato et al.6 reported that the duration of exposure was positively related to cotinine levels, however, most of the studies reported that there was a "poor" agreement between urinary cotinine and self-reported exposure; a self-report assessment of exposure to second-hand smoke in pregnant women misclassified most exposed women as unexposed.7-10
A few studies have examined the association between indoor or outdoor smoking and exposure to second-hand smoke in children.11-13 However, to the best of our knowledge, the association between the area permitted for smoking at home to the smoking family members and positive urinary cotinine, particularly among pregnant nonsmokers, has not yet been reported.
The purpose of this study was to determine the agreement and association between self-reported exposure status to second-hand smoke and positive urinary cotinine levels in pregnant nonsmokers. Furthermore, the association between the area permitted for smoking at home and positive urinary cotinine in pregnant nonsmokers was also examined.
MATERIALS AND METHODS
Study subjects
The study participants included pregnant nonsmokers from the Hallym University Sacred Heart Hospital and 2 community health centers located at Anyang City. The participants visited the prenatal care clinic from December 2005 to March 2006. We asked pregnant nonsmokers who visited the prenatal care clinic whether they would participate in this study and those who voluntarily agreed to do were enrolled. At the time of enrollment, a questionnaire was administered to the participants, and they signed the informed consent. Urine samples were collected in serum separator tubes and stored in the refrigerator and sealed; within a week, the samples were mailed to the clinical laboratory at the National Cancer Center where urinary cotinine levels were measured.
Questionnaire
The questionnaire consisted of 23 items including sociodemographic characteristics and questions related to second-hand smoke exposure. Fig. 1 shows the questions regarding second-hand smoke used in this questionnaire.
Measurement of urinary cotinine
Urinary cotinine levels were measured using the FDA-approved enzyme immunoassay kit and the DRI Cotinine Assay for urine (Microgenics Corp., Fremont, CA, USA) with a Toshiba 200FR (Toshiba Lab Medical, Tokyo, Japan). This kit had a detection limit of 40 ng/mL. The limit of detection (= mean + 3 standard deviation) of 40 ng/mL was determined by 20 replicate measurement of blank. All the tests were performed according to the manufacturer's instructions.
Statistical analyses
We used a dichotomous variable, which was categorized into 2 groups of "pregnant women with positive (≥ 40 ng/mL) and those with negative (< 40 ng/mL) urinary cotinine levels," as the main dependent variable in this study. Fisher's exact test for categorical variables and Wilcoxon's rank sum test for continuous variables were used to test the significance of the baseline differences in the sociodemographic characteristics between the 2 groups. We assessed the agreement between the status of exposure to second-hand smoke as determined by self-report ("Yes" or "No") and by urinary cotinine levels (positive or negative) among the pregnant nonsmokers using the kappa statistic (values ≥ 0.75 were considered as excellent). Using univariable analysis, we assessed the variables associated with positive urinary cotinine level in the subjects who reported living with a smoker. Stepwise multiple logistic regression analyses were performed to assess the association between the independent variables and positive urinary cotinine after adjusting for the confounding variables. All the statistical tests were 2-sided, and p ≤ 0.05 was considered as statistically significant. We used SPSS 12.0K software of Windows for data analyses.
RESULTS
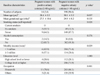
Baseline characteristics of study participants with positive and negative urinary cotinine levels
Table 1 shows the baseline characteristics of the study subjects with positive and negative urinary cotinine. Of the total 412 participants, 14 women (3.4%) showed positive urinary cotinine levels (≥ 40 ng/mL); 305 (74%) had a urinary cotinine concentration of 0 ng/mL, while the rest had urinary cotinine concentrations ranging from 3 ng/mL to 945 ng/mL (Fig. 2). There was a significant difference between the mean ages (standard deviation, SD) of those with positive and negative urinary cotinine levels [28.4 (2.2) and 30.1 (3.2) years, respectively, p = 0.037)]. The mean gestational age showed no significant difference between the 2 groups. The freque-ncy of ex-smokers who had not smoked in the previous month at the time of survey, although they might have smoked earlier, showed a significant difference between the 2 groups, showing 35.7% (5 of 14) and 12.3% (49 of 398), respectively (p = 0.028). The monthly income also showed a significant difference between them. The 2 groups had no significant differences with regard to other characteristics such as alcohol consumption, education level, and occupation.
Agreement between exposure to second-hand smoke as determined by self-report and by urinary cotinine level
Among the participants who reported exposure to second-hand smoke, 4.8% (12 of 249) had cotinine levels of ≥ 40 ng/mL (positive urinary cotinine level), whereas 98.8% (161 of 163) of those who reported no exposure had cotinine levels of < 40 ng/mL (negative urinary cotinine level), and the kappa value was 0.029 (p = 0.049).
Characteristics of the participants who reported exposure to second-hand smoke
The proportion of the participants who reported exposure to second-hand smoke was 60.4% (249 of 412), and these characteristics are presented in Table 2. Among these participants, 27.7% (69 of 249) reported daily exposure to second-hand smoke, and 41.4% (103 of 249) reported exposure in public places such as the cafè. The proportion who reported having a smoker living in the house was 68.3% (170 of 249).
Characteristics of the participants who reported having a smoker living in the house
Among the participants who reported living with a smoker, 90.0% (153 of 170) of those who smoked in the house were their husbands. Among these smokers, 48.2% (82 of 170) smoked ≥ 10 and < 20 cigarettes per day. Among those living with a smoker, 55.9% (95 of 170) reported that smoking was not permitted at home, 38.2% (65 of 170) reported that smoking was allowed in a certain area such as balcony and bathroom, and 5.9% (10 of 170) reported that smoking was allowed in the whole house including bedroom. Most participants (60.6%, 103 of 170) wanted the smoker to quit smoking completely.
Univariable analysis for the variables associated with positive urinary cotinine
In the univariable analysis, "smoking currently permitted in the whole house including bedroom" [(Odds ratio (OR) = 19.93; 95% Confidence interval (CI): 2.84-139.67)] was significantly associated with positive urinary cotinine among the subjects who reported living with the smoker in their family. The association of positive urinary cotinine level with exposure to second-hand smoke (everyday vs. ≤ 6 days, OR = 3.40; 95% CI: 0.92-12.85) was marginally significant. The gestational age and the daily cigarette consumption of smoking of the smoker in the house were not associated with positive urinary cotinine levels.
Stepwise multiple logistic regression analyses for the variables associated with positive urinary cotinine after adjusting for the confounding factors
As shown in Table 3, only "smoking currently permitted in the whole house including the bedroom" was a significant factor of positive urinary cotinine in a stepwise multiple logistic regression analysis after adjusting for the confounding factors such as gestational age, daily cigarette consumption of the smoker in the house, and frequency of exposure to second-hand smoke.
DISCUSSION
We found that the agreement between self-reported exposure to second-hand smoke, as evaluated by using a simple question like "Do you think you are exposed to second-hand smoke?" and positive urinary cotinine in pregnant nonsmokers was poor (kappa value = 0.029). This is similar to the findings of two previous studies of O'Connor et al.7 who measured the urinary cotinine levels and George et al.9 who measured the plasma cotinine that is considered as the gold standard.
Some studies have reported moderate correlations between self-reported exposure to second-hand smoke and urinary cotinine levels.8,14 These controversial findings are due to the fact that there is no well-established and standardized questionnaire presently to investigate the exposure to second-hand smoke during pregnancy. The variables used for the assessment of self-reported exposure to second-hand smoke were different between studies. For example, Rebagliato et al.6 used the number of hours of exposure in the last 3 days; DeLorenze et al.8 used the total number of hours of exposure per day; Kaufman et al.15 used the number of smokers at home (0, 1, and 2+); George et al.9 used the daily exposure to second-hand smoke (≥ 1 hour per day or < 1 hour per day); and the status of exposure to second-hand smoke ("Yes" or "No") was used in the present study. Furthermore, two studies reported that the self-reported information regarding the exposure to second-hand smoke might misclassify a substantial portion of exposed pregnant women as unexposed.8,9 Furthermore, due to the differences in the detectable limit or the cut off limit for cotinine levels for various measurements used in these studies, the positive results of cotinine level could vary between studies.
We also observed that "currently permitted smoking areas at home" was a significant factor of positive urinary cotinine in pregnant nonsmokers. "Smoking currently permitted in the whole house" had a fairly high OR and significant 95% CI for positive urinary cotinine in pregnant nonsmokers when compared with those in whom "smoking was not permitted at home.", although the 95% CI for the variable was rather wide due to the small number of women with positive urinary cotinine. This finding implies that a single question regarding the areas where smoking is permitted at home is a useful way to estimate exposure to second-hand smoke for pregnant nonsmokers living with other smokers. Based on this finding, we suggest that a complete smoking ban at home should be considered to avoid the exposure to second-hand smoke and its potential adverse effects on pregnancy outcomes.
Several studies have reported that the areas where parents smoke at home have a significant association with the urinary cotinine level in children.12,13 To our knowledge, however, the findings in pregnant nonsmokers such as that observed in our study have not previously been reported.
The current study has several limitations. First, we did not enquire about the indoor cigarette consumption of the smokers living. A question regarding daily indoor cigarette consumption of the smokers in each family should be included in a questionnaire because it may not be proportional to the total cigarette consumption per day. Second, we asked respondents to provide limited information regarding the duration of exposure to second-hand smoke such as ≤ 4 hours per day or > 4 hours per day. Detailed information such as the place of exposure as well as concrete exposure hours per day regarding the exposure hours per day on the questionnaire will provide a more accurate analysis of the association between the duration of exposure to second-hand smoke and urinary cotinine. Third, the use of urinary cotinine analysis as the gold standard has been criticized for its short half-life of 3-4 days, interindividual variations, and varied cotinine metabolism during pregnancy.16,17 However, it is unclear whether these factors result in discrepancy between exposure to second-hand smoke as determined by self-report and by urinary cotinine level. Finally, the inclusion of the study participants recruited from a localized area resulted in reduced generalizability of our findings.
In summary, our study indicates that there was poor association between self-reported exposure to second-hand smoke, as evaluated by using a simple question like "Do you think you are exposed to second-hand smoke?" and positive urinary cotinine in pregnant nonsmokers. "Currently permitted smoking areas at home" was a significant factor of positive urinary cotinine in pregnant nonsmokers. We suggest that a question regarding "currently permitted smoking areas at home" should be included in order to evaluate the status of exposure to second-hand smoke in pregnant nonsmokers. Furthermore, a complete smoking ban at home should be considered to avoid potential adverse effects on pregnancy outcomes due to second-hand smoke.




 XML Download
XML Download