

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Transient global amnesia (TGA) is a well known disease that is characterized by a sudden onset of anterograde and retrograde amnesia which persist for less than 24 hours without clouding of consciousness.1 Several potential etiologic factors have been suggested for TGA, including ischemia, seizure, migraine, venous congestion and psychogenic problems.2-8
Although some studies could not find any abnormal lesions with brain MRI, other recent studies showed small, high-signal intensity lesions in the hippocampus using diffusion weighted imaging (DWI).3-5,9,10 Based on these imaging findings, the hypoxic ischemic mechanism was considered as a main etiologic factor.2 However, the detection rate of high-signal intensity lesions on DWI in patients with TGA has variably been reported, ranging from 0 to 84%, and the differences in imaging time after symptom onset, use of serial scans, and different imaging parameters such as slice thickness and a high b value have been suggested to be the reasons for the variation.3,11,12 Because the size of reported hippocampal lesion (1-3 mm) was very small, the imaging method may play an important role in detecting the lesion in TGA.3,11
Since its introduction in clinical practice, high-field strength MRI at 3.0T has shown clinical advantages over 1.5T, especially in the field of neuroradiology.13 Kuhl et al.14 reported that 3.0T DWI increased signal to noise ratio and contrast to noise ratio over 1.5T DWI and detected more ischemic lesions than 1.5T DWI in acute and subacute ischemic stroke patients.
In this study, we retrospectively investigated TGA patients, who underwent 1.5T or 3.0T MRI, to explore the usefulness of high-field strength MRI in detecting probable ischemic lesions in TGA.
MATERIALS AND METHODS
We retrospectively reviewed the patients who met the clinical diagnostic criteria of TGA and brain MRI performed within 5 days after symptom onset.1 Transverse echo-planar DWI was obtained with the following parameters for 1.5T MRI (Vision, Siemens, Erlangen, Germany; TR/TE 5700/139 ms, matrix 64×64, FOV 200×200 mm, slice thickness 5 mm, b = 1,000 s/mm2) and 3.0T (Signa 3.0T, GE, Milwaukee, wis USA; TR/TE 9000/81.4 ms, matrix 128×128, FOV 240×240 mm, slice thickness 4 mm, b = 1,000 s/mm2). The resulting voxel volumes were 49 mm3 and 14 mm3 at 1.5T and 3.0T MRI, respectively.
Acute probable ischemic lesions were defined as regions of high-signal intensity on DWI and corresponding low-signal intensity in apparent diffusion coefficient (ADC) map. A single neuroradiologist blind to clinical history read the images and decided the presence of an acute lesion. Demographic features including amnesia duration and time interval from onset of symptoms to MRI were obtained from medical records and compared them between the 2 groups of different field strength. The presence of vascular risk factors (hypertension, diabetes, smoking, hypercholesterolemia, coronary artery occlusive disease and old cerebrovascular disease) and predisposing factors (emotional stress, physical exertion, and sexual intercourse) were compared between the 2 groups.
Statistical analysis was performed using SPSS 14.0 for Windows. Continuous variables were presented as mean ± SD
and compared with Student's t-test or Mann-Whitney U test based on the normality test using Kolmogorov-Smirnov test. Categorical variables (expressed as counts and percentages) were compared with the Fisher's exact test. A two-tailed value
of p < 0.05 was considered significant.
RESULTS
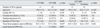
There were total 43 episodes of TGA in 41 patients. Two patients experienced a second amnesic episode at intervals of three and four years; one patient was scanned on 1.5T MRI for both episodes, while the other was scanned on 1.5T for the first episode, and 3.0T for the second episode. Mean age of symptom onset was 60.7 ± 9.6 (range 26-81) years old and 31 patients (75.6%) were female. There were 1 or more vascular risk factors in 21 patients. Mean duration of amnesia was 6.1 ± 3.7 hours (range 1-13), and mean time interval from symptom onset to brain MRI was 37.9 ± 23.9 hours (range 4-120). Eleven episodes were examined with a 1.5T MRI and 32 episodes were examined with 3.0T MRI. Eleven out of 32 patients (34.4%) who were examined with 3.0T MRI showed high-signal intensity lesions on DWI with corresponding low-signal intensity on ADC map in the hippocampus unilaterally [(5 in right, 4 in left) or bilaterally in 2 (Fig. 1)]. The mean size of the lesions was small (2.8 ± 0.6 mm) on transverse DWI. On the contrary, no lesion was found in 11 patients who were examined with 1.5T MRI. There were no significant differences in age, gender, vascular risk factor, predisposing factor, duration of amnesia, and time interval from onset of symptom to brain MRI between the patients examined with 1.5 and 3.0T MRI (Table 1).
In 32 patients who were tested with 3.0T DWI, there were no significant differences between the patients with visible DWI lesion and those without it in age, gender, vascular risk factor, predisposing factor, duration of amnesia, and time interval from onset of symptom to brain MRI.
DISCUSSION
In this study, none of 11 patients who were examined with 1.5T MRI showed acute probable ischemic lesions on DWI. However, 11 out of 32 patients who were examined with 3.0T MRI showed small hyperintense lesions in the hippocampus on DWI with corresponding low-signal intensity on ADC map. All lesions were located in memory-related structures, compatible with the previous reports. There were no significant differences in demographic and clinical variables between the group examined with 1.5T MRI and the group examined with 3.0T MRI.
It is tempting to attribute the difference in the detection rate found between the two scanners to the difference in magnetic field strength. However, the two systems differ in other aspects also: their age and the technology available at the time they were introduced. Aside from field strength, the most notable difference is the performance of the gradient subsystem which impacts the quality of echo planar images, and in particular, DWI. With the improved gradient subsystem, the in-plane resolution can be increased, reducing voxel size, while the echo time of the DWI sequence can be decreased, thus further increasing signal to noise ratio. Due to these differences, the DWI images used in our routine clinical care have significantly smaller voxel size (14 mm3 on the 3.0T compared to 49 mm3 on the 1.5T), while the signal to noise remains similar. We speculate that the increased resolution realized by the current generation 3.0T MRI made the differences in lesion detection rate between the two groups. Previous reports suggested that subtle changes on 1.5T DWI were missed during the first read, however, were correctly diagnosed by the second read or follow up MRI.3,11 One can reduce the voxel size on 1.5T MRI to that of 3.0T MRI. However, it would be limited by low-signal to noise and contrast to noise ratio, which makes lesions less conspicuous than 3.0T MRI with the same voxel size.
When compared the DWI parameters of our study with previous reports which showed ischemic lesions on 1.5T MRI, we found that the voxel size of our 1.5T DWI (49 mm3) was larger than the others (12-18 mm3). Since most of the lesions reported in TGA are very small, a large voxel size might have difficulty in detecting a lesion by partial volume effect, unless the lesion was centered in a single voxel. High resolution DWI using a different imaging sequence in 1.5T MRI was reported to detect more cortical lesion in acute ischemic stroke.15,16 Furthermore, acquirement of serial MRI scans and other image sections, such as coronal, in addition to transverse images could increase the detection rate of DWI lesions. We suspect that these are the main causes of no lesion detection in our 1.5T MRI study.
Bartsch et al.17 performed 3.0T MRI in TGA patient within 72 hours after symptom onset and reported that DWI lesions were detected in 29 out of 42 episodes (69%) of TGA, which was much higher than our results (34.3%). We speculate that the use of small voxel size (4.7 mm3), serial MRI scans and additional coronal section image might have contributed to the high detectibility of DWI lesion. In 32 patients with 3.0T MRI, we could not find any differences in demographic and clinical variables between patients with and without probable ischemic lesions. However, if we tried to detect probable ischemic lesion in a larger number of patients by using serial scans, thin slice thickness and additional image sections, we might be able to find a more accurate correlation between the clinical characteristics of TGA and presence of probable ischemic lesions.
Our study has a limitation. Although we showed no differences in baseline characteristics between the groups of 1.5 and 3.0T MRI, our results showed only indirect evidence to indicate superiority of high-field strength MRI over low-field strength.
In conclusion, we found that the detectibility of DWI lesion in TGA is dependent on the sensitivity of the MR scanner and MR sequence. Because of previous findings in TGA, such as small lesion size and delayed MR changes after onset, more precise and proper diagnostic methods such as high-field strength MRI, refined sequence parameters and serial MRI scans are needed to investigate the exact pathomechanism of TGA.

 XML Download
XML Download