

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The reported incidence of coronary anomalies is approximately 1%. However, the incidence was found to be 5.6% in a recent prospective angiographic study of 1,950 consecutive cases.1 Among these cases, an anomalous right coronary artery (RCA) from the left sinus was found in approximately 0.03 - 0.9% of patients undergoing coronary angiography.2 An anomalous origin of the RCA from the ascending aorta above the left sinus is associated with angina pectoris, acute myocardial infarction or sudden cardiac arrest when it courses between the aorta and the pulmonary trunk. A case of an anomalous origin of the left coronary artery (LCA) from the posterior sinus is extremely rare.
We present a case of a RCA, in which an anomalous right coronary artery arises from the ascending aorta above the left sinus of Valsalva and courses between the aorta and pulmonary trunk. Additionally, this individual had an acute myocardial infarction of the inferior wall and an anomalous origin of the LCA from the posterior sinus of Valsalva.
CASE REPORT
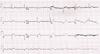
A 54-year-old man arrived at the emergency room in an inebriated state complaining of left shoulder pain accompanied by headache. His risk factors included smoking one-half of a pack of cigarettes per day over a 20-year period and a 10-year history of hypertension. Physical examination revealed a blood pressure of 70/40 mmHg and a pulse rate of 40 beats per minute. His limbs were cold and clammy. There were no abnormal cardiac or respiratory sounds. Electrocardiography revealed Q waves and 2-mm to 3-mm elevations of the ST segment in II, III and aVF and 3:1 AV block (Fig. 1), indicating an acute myocardial infarction involving the inferior wall. An echocardiogram revealed akinesia of the inferior wall and a mildly depressed left ventricular ejection fraction of 47%. His cardiac enzyme levels, such as creatine kinase-MB and cardiac troponin-I, were elevated to 60.1 ng/mL and 27 ng/mL, respectively. Blood urea nitrogen and serum creatinine also were elevated to 34 mg/dL and 2.6 mg/dL, respectively.
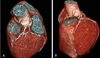
He was implanted with a transvenous temporary pacemaker and an emergency direct coronary angiography was performed. However, in the first trial the LCA could not be selectively cannulated with Judkins left (JL) or Amplantz left (AL) catheter and the RCA could not be selectively cannulated with Judkins right (JR) catheter, Amplantz right (AR) catheter, or the AL catheter. Nonselective coronary angiography was performed by ascending aortography, and this revealed TIMI III distal flow of the RCA. Also, the LCA and RCA were suspected to originate from the left sinus of the Valsalva. During angiography, the patient's chest pain subsided spontaneously, his vital signs were stabilized, and he recovered from the 3 : 1 AV block and returned to sinus rhythm. Due to transient acute renal failure, the initial serum creatinine level was too high to use a radiocontrast for taking multi-detector computerized tomography (MDCT). Therefore we waited and serially monitored the level until it normalized. On the third hospital day, MDCT revealed an anomalous origin of the RCA from the ascending aorta above the left sinus of Valsalva and the LCA from the posterior sinus of Valsalva (Fig. 2). The RCA coursed between the ascending aorta and the pulmonary trunk, and significant narrowing was observed at the junctional point between the portion wrapped around the aorta, pulmonary artery and the free portion of the proximal RCA, and middle RCA.
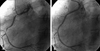
On the seventh hospital day, a second trial of coronary angiography was performed. After confirming the absence of a right coronary artery ostium on the right sinus of Valsalva, the anomalous RCA was selectively cannulated with a 6Fr AL1 guiding catheter. The coronary angiography revealed a tubular eccentric proximal RCA with 95% stenosis and a thrombus, and a diffuse, irregular middle RCA with up to 95% stenosis (Fig. 3). The lesions were crossed with a Hi-torque PILOT 0.014 guidewire (Guidant). The AL1 catheter offered stable seating and superior back-up support. A 2.5 × 20mm Ryujin plus (Terumo) balloon dilatation was performed at the proximal RCA and middle RCA lesions. A 3.5 × 16 mm TAXUS stent (Tax, Boston scientific, Natick, MA, USA) was successfully deployed in the proximal RCA lesion and a 3.0 × 28 mm TAXUS stent (Boston scientific) was deployed in the middle RCA lesion. A final angiogram revealed that the procedure was successful (Fig. 3). A left coronary angiogram performed using a 5Fr AR2 catheter showed no significant narrowing of the LCA, which originated from the posterior sinus of Valsalva (Fig. 4). The patient was discharged on the tenth day.
DISCUSSION
The prevalence of an anomalous origin of a coronary artery from the opposite sinus (ACAOS) is unclear. A recent prospective angiographic study reported the incidence as 1.07%, which included a 0.92% rate of ectopic RCA originating from the left sinus and a 0.15% rate of ectopic LCA arising from the right sinus.1
An anomalous RCA might originate from the anterior aspect of the ascending aorta usually above the sinotubular line (high anterior take-off), from the left sinus of Valsalva with a separate ostium from the left main coronary artery, from the left main coronary artery (as a single coronary artery), or from the pulmonary trunk.
It is well known that an anomalous origin of the RCA can lead to angina pectoris, a myocardial infarction, ventricular tachycardia, ventricular fibrillation, syncope and sudden death.
The pathophysiological mechanism of these clinical phenomena is still a concern. However, the usual explanation is the mechanical compression of the right coronary artery by the great vessels, the aorta and the pulmonary artery. In addition, an abnormal slit-like RCA ostium in the aortic wall and an acute angulation of the RCA can lead to these pathologic results. Hutchins et al.2 suggested that the unusual angle of take-off and the more tortuous course of the proximal portion of the anomalous coronary artery can accelerate the rate of atherosclerosis. Liu et al.3 suggested that the junction point of the bound portion and the free portion of an anomalous artery as it wraps around the aorta is an area that is susceptible to lipid accumulation. These mechanisms can explain the obstructive lesion in the coronary artery of our patient.
It is important to identify the culprit vessel as soon as possible in an acute myocardial infarction. However, in a patient with a coronary artery with an anomalous origin, it is difficult to quickly and precisely cannulate all three coronary arteries and to determine the subsequent treatment strategy. The selective cannulation of anomalous arteries can be a formidable challenge due to the unusual ostial location, take-off orientation and aberrant course of the artery.
Some authors emphasize the importance of selecting a guiding catheter by "trial and error." Hon-Kan et al.4 suggested that Amplatz guiding catheters be considered when an anomalous-origin RCA has an anterior-superior take-off because these catheters offer stable seating and superior back-up support. However, if an anomalous-origin RCA arises from the left sinus of Valsalva, one should first consider Judkins left guiding catheters with a secondary curve 0.5 cm longer than the diagnostic catheter for the left coronary artery. This is because they can easily be manipulated through clockwise or counter-clockwise rotation and usually are able to engage the RCA without any difficulty under a fluoroscope by the lateral view.
At coronary angiography, the precise course of the anomalous vessel may be difficult to delineate due to its complex three-dimensional geometry shown in two dimensions fluoroscopically. One study used multidetector computed tomography (MDCT) to image the monocuspal origin of all three coronary arteries from the right sinus.5
In our case, MDCT was found to be a useful, accurate, and convenient complementary tool for coronary angiography. Although there are some limitations in using this diagnostic modality in urgent direct PTCA cases, it is a valuable tool for precisely depicting the anomalous origin and relationships between the coronary vessel, great vessel, and ventricles.
Although this topic is still open in cardiology, the right coronary artery originating from the left coronary sinus is a more common anomaly, and its prognosis and treatment are better known than for other coronary anomalies. It should be noted that in our case, the LCA originated from the posterior sinus. Left ACAOS is less frequent and its treatment is less clearly defined.
A case of a coronary artery anomaly involving more than one coronary artery is quite rare. Fineschi M. reported a rare case of the anomalous origin of all three major coronary arteries from the right sinus, which included the anomalous origin of LCX and the common origin of the LAD and RCA.6 To our knowledge, our coronary anomaly, in which the RCA originated from the left sinus and the LCA originated from the right sinus separately, is the first case reported.
We report using MDCT to successfully treat an inferior wall myocardial infarction with an uncommon coronary artery anatomy, where the RCA originated above the left coronary sinus of Valsalva and the LCA originated separately from the posterior coronary sinus of Valsalva. The rarity and clinical significance of this case are emphasized.

 XML Download
XML Download